

Surgery for synchronous and metachronous single-organ metastasis of pancreatic cancer: a SEER database analysis and systematic literature review
- PMID: 32157155
- PMCID: PMC7064579
- DOI: 10.1038/s41598-020-61487-0
Surgery for synchronous and metachronous single-organ metastasis of pancreatic cancer: a SEER database analysis and systematic literature review
Abstract
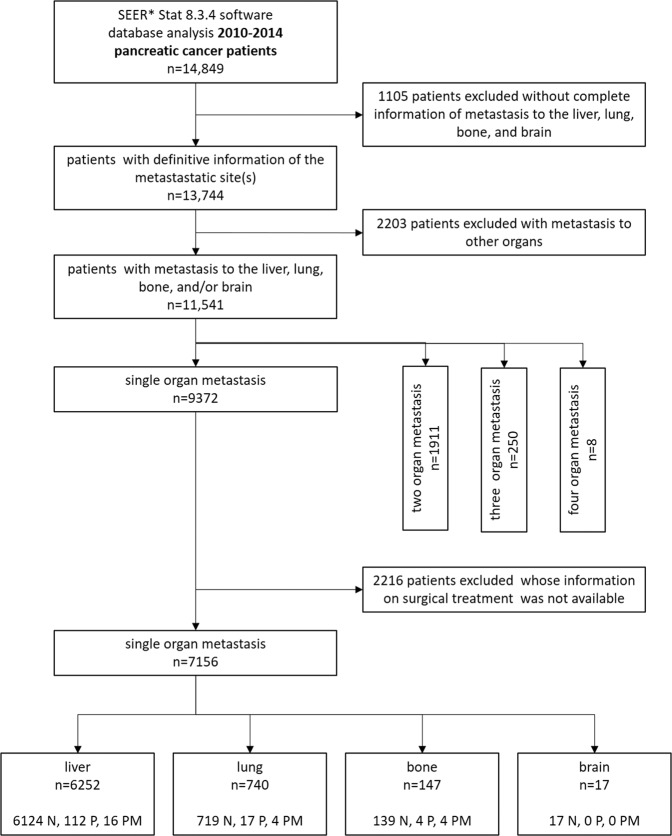
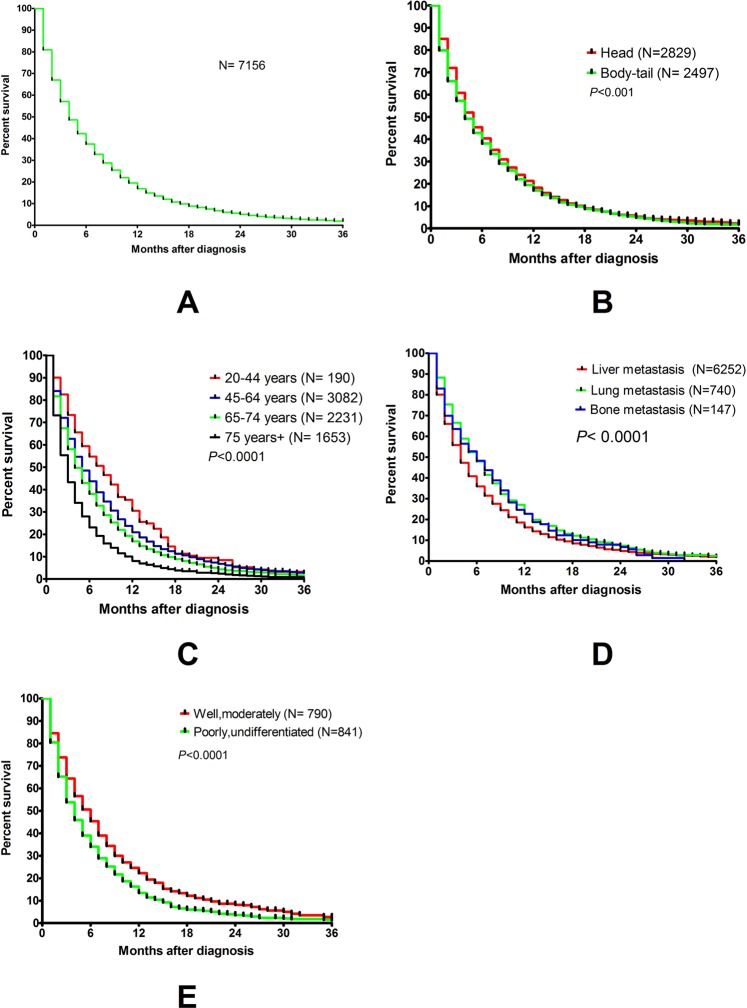
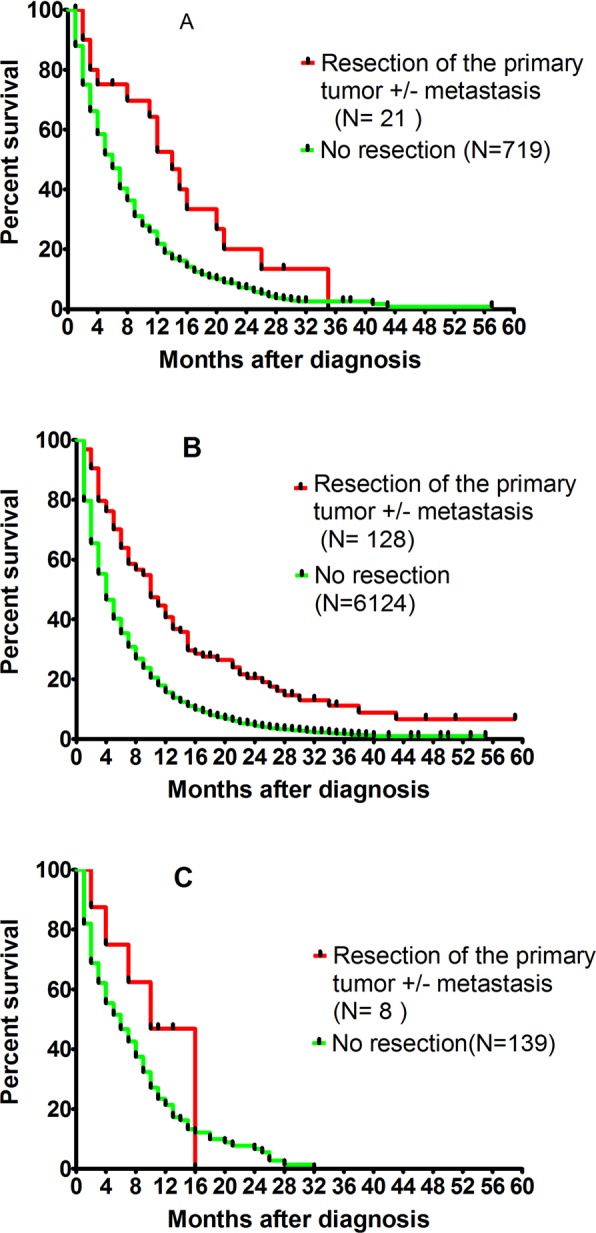
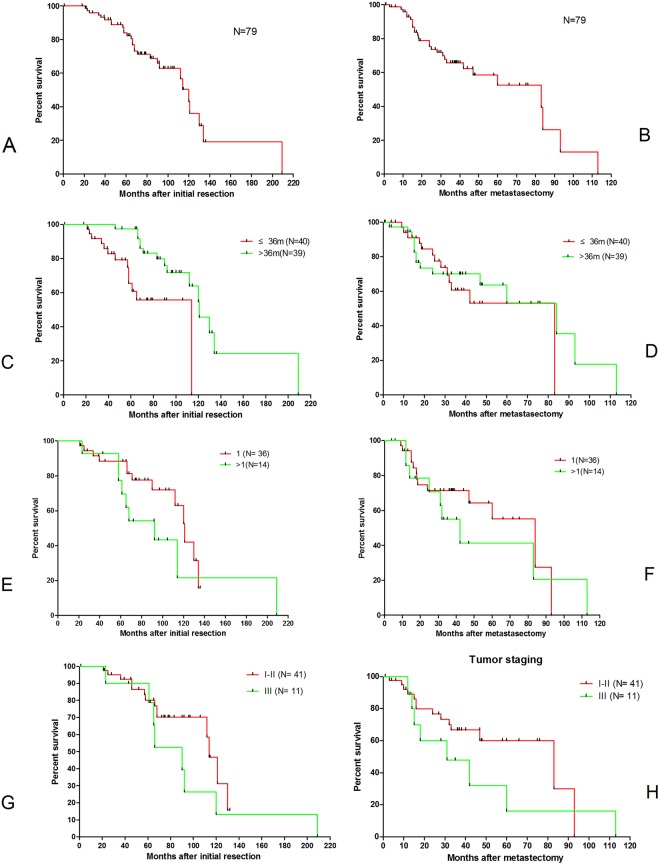
Surgery for metastatic pancreatic cancer remains controversial as the survival benefit is questionable. The aim of the present study was to analyze the survival of these patients using data extracted from the surveillance, epidemiology, and end results (SEER) program database. Further, studies on resection for metastatic disease to the lung were systematically reviewed. A total of 11,541 cases with synchronous distant metastasis were analyzed. The median survival of single-organ metastasis was better than of multi-organ metastasis (single-organ 4.0 ± 0.07 months, two-organs 3.0 ± 0.13 months, three/four-organs 2.0 ± 0.19 months; p < 0.0001). Single organ lung metastasis had longer median survival times compared to the other sites (lung 6.0 ± 0.32 months, HR 0.87, 95% CI 0.78-0.97; p = 0.013). Resection of the primary tumor was associated with longer survival in synchronous single-organ metastasis to the lung compared to no resection (14.0 ± 1.93 months vs 6.0 ± 0.31 months, p < 0.0001). A systematic literature review identified 79 cases of metachronous lung metastasis with a survival of 120.0 ± 6.32 months and 83.0 ± 24.84 months following resection of the primary tumor and metastasis, respectively. Lower TNM staging, longer interval to metastasis, and single metastatic lesion correlated with better survival. Resection in highly selected pancreatic cancer patients with synchronous and metachronous lung only metastasis might confer a survival benefit and should be considered on an individual basis.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Maeda S, Unno M, Yu J. Adjuvant and neoadjuvant therapy for pancreatic cancer. J. Pancreatology. 2019;2:100–106. doi: 10.1097/jp9.0000000000000028. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
