

Slow progressors to type 1 diabetes lose islet autoantibodies over time, have few islet antigen-specific CD8+ T cells and exhibit a distinct CD95hi B cell phenotype
- PMID: 32157332
- PMCID: PMC7228996
- DOI: 10.1007/s00125-020-05114-7
Slow progressors to type 1 diabetes lose islet autoantibodies over time, have few islet antigen-specific CD8+ T cells and exhibit a distinct CD95hi B cell phenotype
Abstract
Aims/hypothesis: The aim of this study was to characterise islet autoantibody profiles and immune cell phenotypes in slow progressors to type 1 diabetes.
Methods: Immunological variables were compared across peripheral blood samples obtained from slow progressors to type 1 diabetes, individuals with newly diagnosed or long-standing type 1 diabetes, and healthy individuals. Polychromatic flow cytometry was used to characterise the phenotypic attributes of B and T cells. Islet autoantigen-specific B cells were quantified using an enzyme-linked immunospot (ELISpot) assay and islet autoantigen-specific CD8+ T cells were quantified using peptide-HLA class I tetramers. Radioimmunoassays were used to detect islet autoantibodies. Sera were assayed for various chemokines, cytokines and soluble receptors via ELISAs.
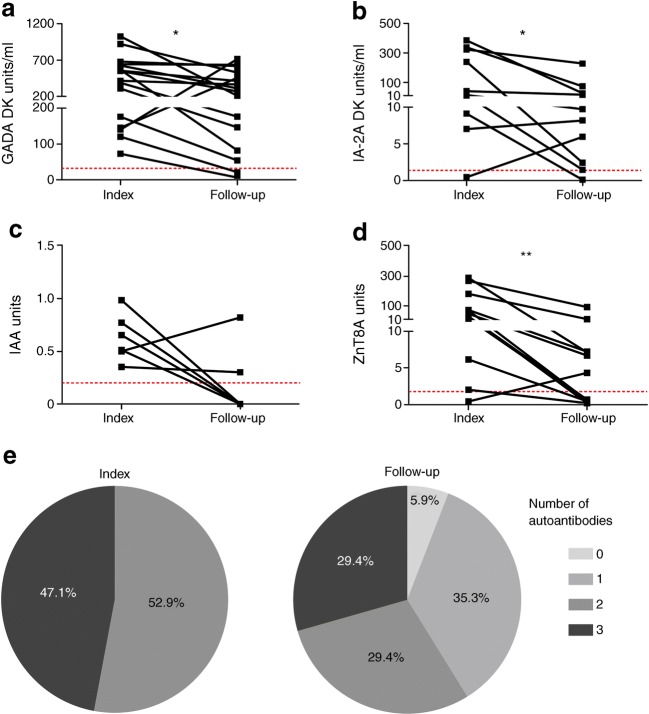
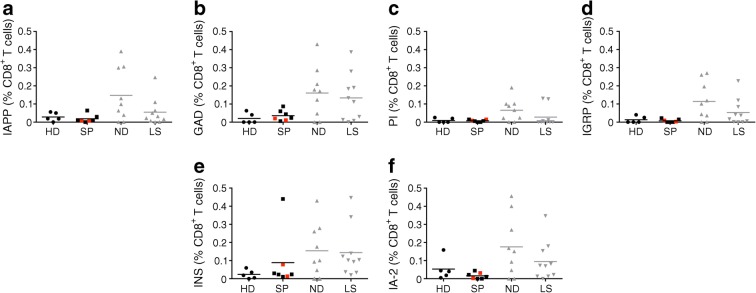
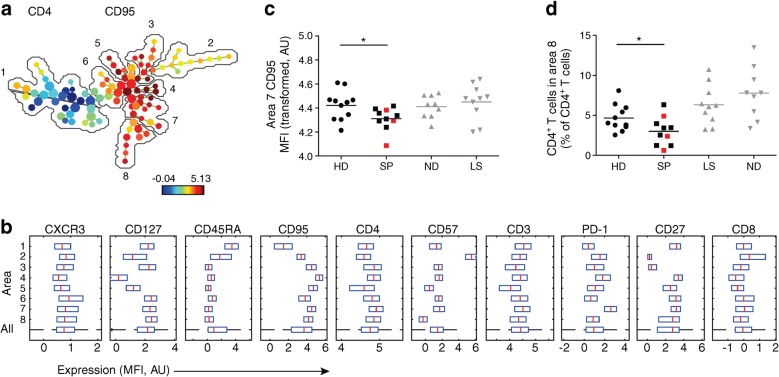
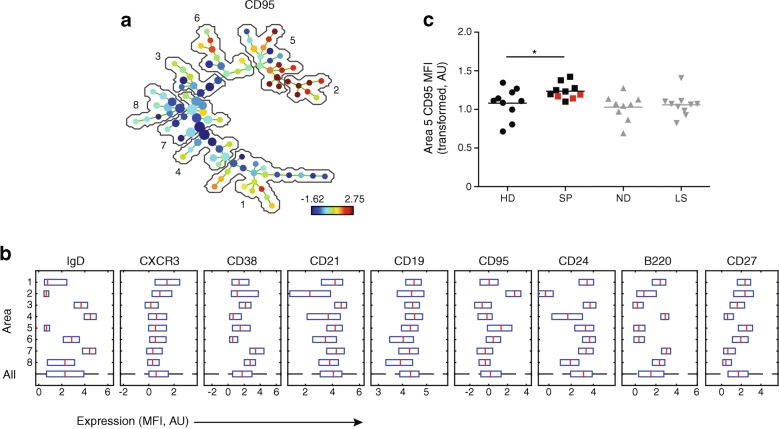
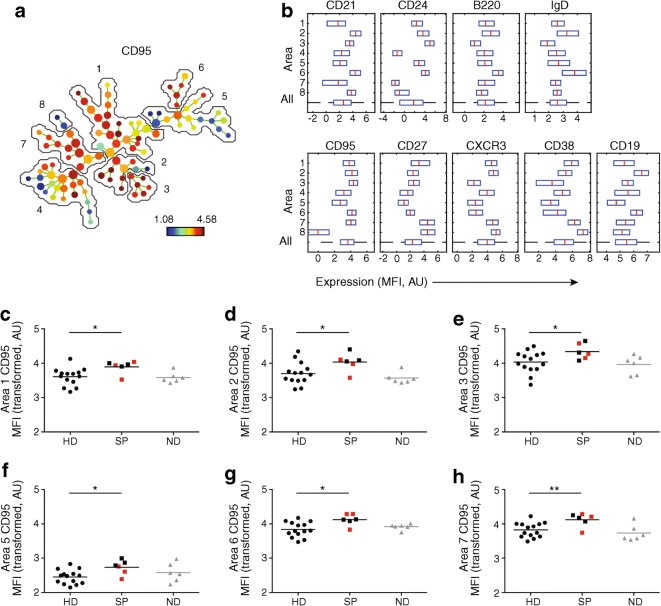
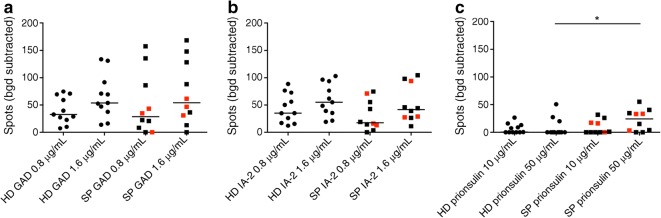
Results: Islet autoantibodies were lost over time in slow progressors. Various B cell subsets expressed higher levels of CD95 in slow progressors, especially after polyclonal stimulation, compared with the corresponding B cell subsets in healthy donors (p < 0.05). The phenotypic characteristics of CD4+ and CD8+ T cells were similar in slow progressors and healthy donors. Lower frequencies of CD4+ T cells with a central memory phenotype (CD27int, CD127+, CD95int) were observed in slow progressors compared with healthy donors (mean percentage of total CD4+ T cells was 3.00% in slow progressors vs 4.67% in healthy donors, p < 0.05). Autoreactive B cell responses to proinsulin were detected at higher frequencies in slow progressors compared with healthy donors (median no. of spots was 0 in healthy donors vs 24.34 in slow progressors, p < 0.05) in an ELISpot assay. Islet autoantigen-specific CD8+ T cell responses were largely absent in slow progressors and healthy donors. Serum levels of DcR3, the decoy receptor for CD95L, were elevated in slow progressors compared with healthy donors (median was 1087 pg/ml in slow progressors vs 651 pg/ml in healthy donors, p = 0.06).
Conclusions/interpretation: In this study, we found that slow progression to type 1 diabetes was associated with a loss of islet autoantibodies and a distinct B cell phenotype, consistent with enhanced apoptotic regulation of peripheral autoreactivity via CD95. These phenotypic changes warrant further studies in larger cohorts to determine their functional implications.
Keywords: Autoantibodies; B cells; CD95; DcR3; ELISpot; Peptide-HLA class I tetramers; Proinsulin; Slow progressors to type 1 diabetes; T cells.
Figures
Similar articles
-
Activated but functionally impaired memory Tregs are expanded in slow progressors to type 1 diabetes.Diabetologia. 2022 Feb;65(2):343-355. doi: 10.1007/s00125-021-05595-0. Epub 2021 Oct 28. Diabetologia. 2022. PMID: 34709423 Free PMC article.
-
Characteristics of slow progression to diabetes in multiple islet autoantibody-positive individuals from five longitudinal cohorts: the SNAIL study.Diabetologia. 2018 Jun;61(6):1484-1490. doi: 10.1007/s00125-018-4591-5. Epub 2018 Mar 12. Diabetologia. 2018. PMID: 29532109 Free PMC article.
-
CD8 T-cell reactivity to islet antigens is unique to type 1 while CD4 T-cell reactivity exists in both type 1 and type 2 diabetes.J Autoimmun. 2014 May;50:77-82. doi: 10.1016/j.jaut.2013.12.003. Epub 2013 Dec 30. J Autoimmun. 2014. PMID: 24387802
-
What Have Slow Progressors Taught Us About T1D-Mind the Gap!Curr Diab Rep. 2019 Sep 10;19(10):99. doi: 10.1007/s11892-019-1219-1. Curr Diab Rep. 2019. PMID: 31501992 Free PMC article. Review.
-
The potential of multimer technologies in type 1 diabetes prediction strategies.Diabetes Metab Res Rev. 2011 Mar;27(3):216-29. doi: 10.1002/dmrr.1165. Diabetes Metab Res Rev. 2011. PMID: 21309048 Review.
Cited by
-
Cellular zinc metabolism and zinc signaling: from biological functions to diseases and therapeutic targets.Signal Transduct Target Ther. 2024 Jan 3;9(1):6. doi: 10.1038/s41392-023-01679-y. Signal Transduct Target Ther. 2024. PMID: 38169461 Free PMC article. Review.
-
The many faces of islet antigen-specific CD8 T cells: clues to clinical outcome in type 1 diabetes.Immunol Cell Biol. 2021 May;99(5):475-485. doi: 10.1111/imcb.12437. Epub 2021 Feb 21. Immunol Cell Biol. 2021. PMID: 33483981 Free PMC article. Review.
-
Consensus Guidance for Monitoring Individuals With Islet Autoantibody-Positive Pre-Stage 3 Type 1 Diabetes.Diabetes Care. 2024 Aug 1;47(8):1276-1298. doi: 10.2337/dci24-0042. Diabetes Care. 2024. PMID: 38912694 Free PMC article. Review.
-
Activated but functionally impaired memory Tregs are expanded in slow progressors to type 1 diabetes.Diabetologia. 2022 Feb;65(2):343-355. doi: 10.1007/s00125-021-05595-0. Epub 2021 Oct 28. Diabetologia. 2022. PMID: 34709423 Free PMC article.
-
Insights From Single Cell RNA Sequencing Into the Immunology of Type 1 Diabetes- Cell Phenotypes and Antigen Specificity.Front Immunol. 2021 Oct 1;12:751701. doi: 10.3389/fimmu.2021.751701. eCollection 2021. Front Immunol. 2021. PMID: 34659258 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
