

Clinical, procedural and long-term outcome of ischemic VT ablation in patients with previous anterior versus inferior myocardial infarction
- PMID: 32157380
- PMCID: PMC7515937
- DOI: 10.1007/s00392-020-01622-z
Clinical, procedural and long-term outcome of ischemic VT ablation in patients with previous anterior versus inferior myocardial infarction
Abstract
Background: Outcome of ischemic VT ablation may differ between patients with previous myocardial infarction (MI) in relation to infarct localization.
Methods: We analyzed procedural data, acute and long-term outcomes of 152 consecutive patients (139 men, mean age 67 ± 9 years) with previous anterior or inferior MI who underwent ischemic VT ablation at our institution between January 2010 and October 2015.
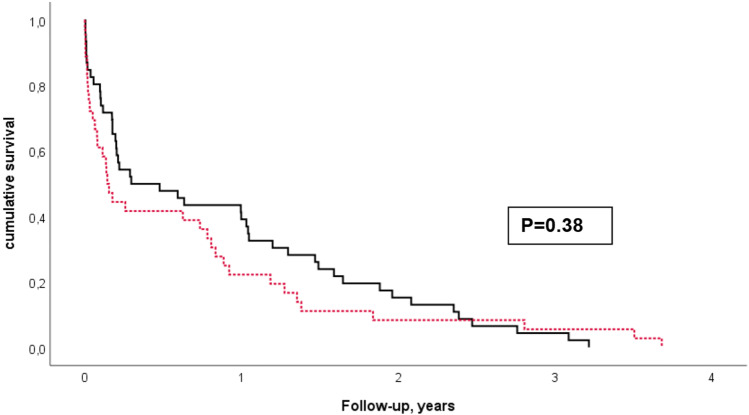
Results: More patients had a history of inferior MI (58%). Mean ejection fraction was significantly lower in anterior MI patients (28 ± 10% vs. 34 ± 10%, p < 0.001). NYHA class and presence of comorbidities were not different between the groups. Indication for the procedure was electrical storm in 43% of patients, and frequent implantable cardioverter defibrillator (ICD) therapies in 57%, and did not differ significantly between anterior and inferior MI patients. A mean of 3 ± 2 VT morphologies were inducible, with a trend towards more VT in the anterior MI group (3.1 ± 2.2 vs. 2.6 ± 1.9, p = 0.18). Procedural parameters and acute success did not differ between the groups. During a mean follow-up of 3 ± 2 years, more anterior MI patients had undergone a re-ablation (49% vs. 33%, p = 0.09, Chi-square test). There was a trend towards more ICD shocks in patients with previous anterior MI (46% vs. 34%). After adjusting for risk factors and ejection fraction, multivariable Cox regression analyses showed no significant difference in mortality (p = 0.78) and cardiovascular mortality between infarct localizations (p = 0.6).
Conclusion: Clinical characteristics of patients with anterior and inferior MI are similar except for ejection fraction. Patients with inferior MI appear to have better outcome regarding survival, ICD shocks and re-ablation, but this appears to be related to better ejection fraction when compared with anterior MI.
Keywords: Catheter ablation; Ischemic cardiomyopathy; Localization of scar; Ventricular tachycardia.
Figures

References
-
- Priori SG, Blomström-Lundqvist C, Mazzanti A, et al. ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC) Eur Heart J. 2015;36:2793–2867. doi: 10.1093/eurheartj/ehv316. - DOI - PubMed
-
- Tung R, Vaseghi M, Frankel DS, et al. Freedom from recurrent ventricular tachycardia after catheter ablation is associated with improved survival in patients with structural heart disease: an International VT Ablation Center Collaborative Group study. Heart Rhythm. 2015;12:1997–2007. doi: 10.1016/j.hrthm.2015.05.036. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
