

Drug-Drug Interactions with Direct Oral Anticoagulants
- PMID: 32157630
- PMCID: PMC7403169
- DOI: 10.1007/s40262-020-00879-x
Drug-Drug Interactions with Direct Oral Anticoagulants
Erratum in
-
Correction to: Drug-Drug Interactions with Direct Oral Anticoagulants.Clin Pharmacokinet. 2020 Dec;59(12):1647. doi: 10.1007/s40262-020-00954-3. Clin Pharmacokinet. 2020. PMID: 33125627 Free PMC article.
Abstract
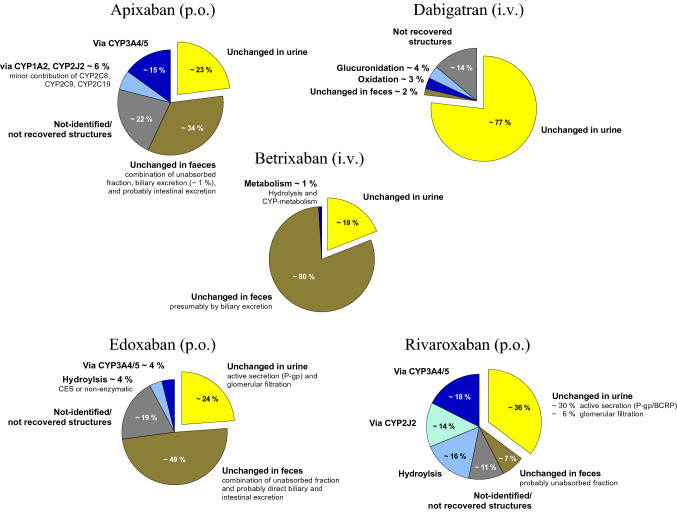
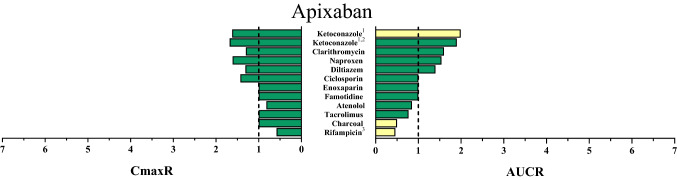
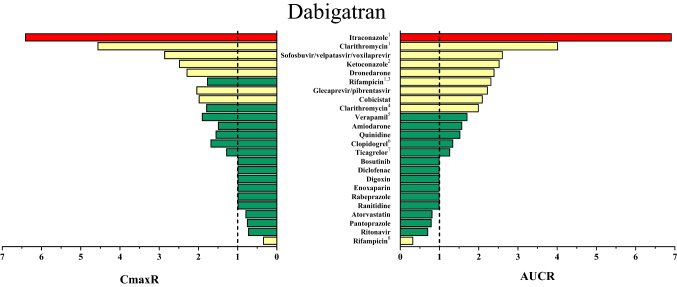
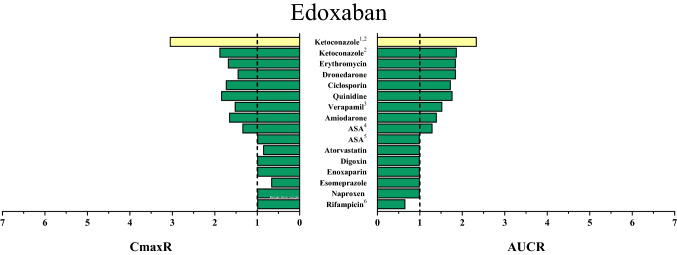
A large body of evidence suggests that not only direct anticoagulant effects but also major bleeding events and stroke prevention depend on plasma concentrations of direct oral anticoagulants (DOACs). Concomitant drugs that cause drug-drug interactions (DDIs) alter DOAC exposure by increasing or decreasing DOAC bioavailability and/or clearance; hence, they might affect the efficacy and safety of DOAC therapy. Patients with renal impairment already receive smaller DOAC maintenance doses because avoidance of elevated DOAC exposure might prevent serious bleeding events. For other causes of increased exposure such as DDIs, management is often less well-defined. Considering that DOAC patients are often older and have multiple co-morbidities, polypharmacy is highly prevalent. However, the effect of multiple drugs on DOAC exposure, and especially the impact of DDIs when concurring with drug-disease interactions as observed in renal impairment, has not been thoroughly elucidated. In order to provide effective and safe anticoagulation with DOACs, understanding the mechanisms and magnitude of DDIs appears relevant. Instead of avoiding drug combinations with DOACs, more DDI trials should be conducted and new strategies such as dose adjustments based on therapeutic drug monitoring should be investigated. However, dose adjustments based on concentration measurements cannot currently be recommended because evidence-based data are missing.
Conflict of interest statement
KIF and SH declare that they have no potential conflicts of interest that might be relevant to the contents of this manuscript. GM received consulting honoraria and data and safety monitoring board honoraria from Boehringer Ingelheim and Bayer outside the submitted work. WEH received consulting honoraria, speaker’s honoraria, and travel support from BMS, Boehringer Ingelheim, and Daiichi Sankyo and research support from Bayer and Daichii-Sankyo outside the submitted work.
Figures

References
-
- U.S. Food and Drug Administration. Betrixaban: clinical pharmacology and biopharmaceutics review; 2016. https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/208383Orig1s000C.... Accessed 29 Jan 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
