

min-SIA: a Lightweight Algorithm to Predict the Risk of 6-Month Mortality at the Time of Hospital Admission
- PMID: 32157649
- PMCID: PMC7210334
- DOI: 10.1007/s11606-020-05733-1
min-SIA: a Lightweight Algorithm to Predict the Risk of 6-Month Mortality at the Time of Hospital Admission
Abstract
Background: Predicting death in a cohort of clinically diverse, multi-condition hospitalized patients is difficult. This frequently hinders timely serious illness care conversations. Prognostic models that can determine 6-month death risk at the time of hospital admission can improve access to serious illness care conversations.
Objective: The objective is to determine if the demographic, vital sign, and laboratory data from the first 48 h of a hospitalization can be used to accurately quantify 6-month mortality risk.
Design: This is a retrospective study using electronic medical record data linked with the state death registry.
Participants: Participants were 158,323 hospitalized patients within a 6-hospital network over a 6-year period.
Main measures: Main measures are the following: the first set of vital signs, complete blood count, basic and complete metabolic panel, serum lactate, pro-BNP, troponin-I, INR, aPTT, demographic information, and associated ICD codes. The outcome of interest was death within 6 months.
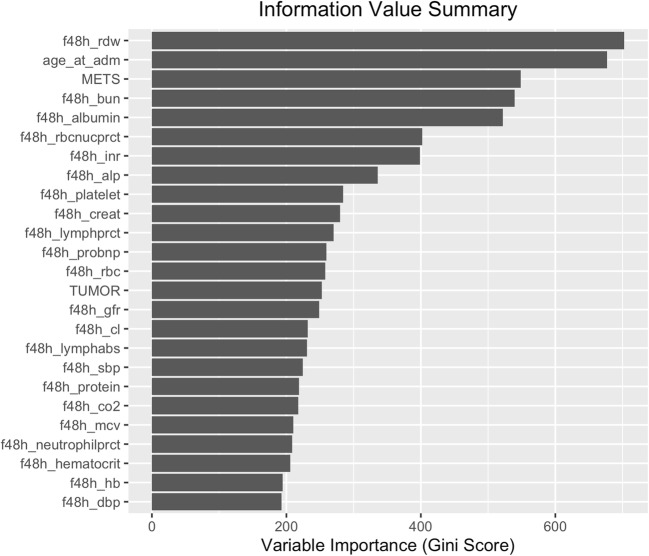
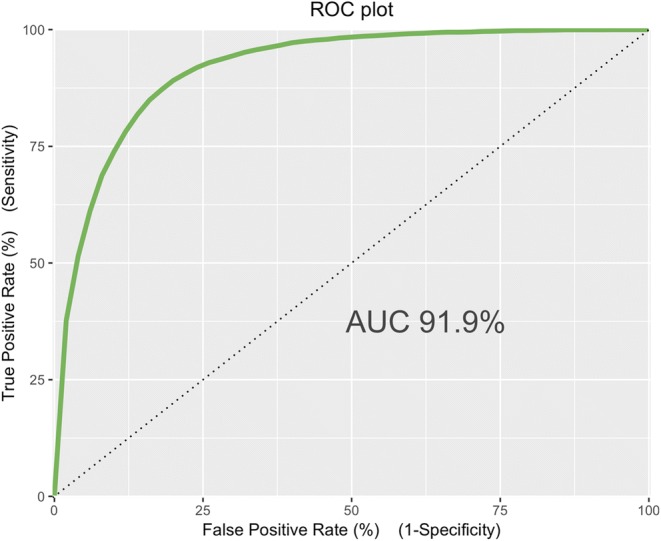
Key results: Model performance was measured on the validation dataset. A random forest model-mini serious illness algorithm-used 8 variables from the initial 48 h of hospitalization and predicted death within 6 months with an AUC of 0.92 (0.91-0.93). Red cell distribution width was the most important prognostic variable. min-SIA (mini serious illness algorithm) was very well calibrated and estimated the probability of death to within 10% of the actual value. The discriminative ability of the min-SIA was significantly better than historical estimates of clinician performance.
Conclusion: min-SIA algorithm can identify patients at high risk of 6-month mortality at the time of hospital admission. It can be used to improved access to timely, serious illness care conversations in high-risk patients.
Keywords: data mining; hospital outcomes; palliative care; predictive models.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures

Similar articles
-
Development and Validation of Machine Learning Models for Prediction of 1-Year Mortality Utilizing Electronic Medical Record Data Available at the End of Hospitalization in Multicondition Patients: a Proof-of-Concept Study.J Gen Intern Med. 2018 Jun;33(6):921-928. doi: 10.1007/s11606-018-4316-y. Epub 2018 Jan 30. J Gen Intern Med. 2018. PMID: 29383551 Free PMC article.
-
Development and Validation of an Electronic Health Record-Based Machine Learning Model to Estimate Delirium Risk in Newly Hospitalized Patients Without Known Cognitive Impairment.JAMA Netw Open. 2018 Aug 3;1(4):e181018. doi: 10.1001/jamanetworkopen.2018.1018. JAMA Netw Open. 2018. PMID: 30646095 Free PMC article.
-
Dynamic and explainable machine learning prediction of mortality in patients in the intensive care unit: a retrospective study of high-frequency data in electronic patient records.Lancet Digit Health. 2020 Apr;2(4):e179-e191. doi: 10.1016/S2589-7500(20)30018-2. Epub 2020 Mar 12. Lancet Digit Health. 2020. PMID: 33328078
-
A deep attention model to forecast the Length Of Stay and the in-hospital mortality right on admission from ICD codes and demographic data.J Biomed Inform. 2021 Jun;118:103778. doi: 10.1016/j.jbi.2021.103778. Epub 2021 Apr 17. J Biomed Inform. 2021. PMID: 33872817
-
A Real-Time Early Warning System for Monitoring Inpatient Mortality Risk: Prospective Study Using Electronic Medical Record Data.J Med Internet Res. 2019 Jul 5;21(7):e13719. doi: 10.2196/13719. J Med Internet Res. 2019. PMID: 31278734 Free PMC article.
References
-
- Curtis JR, Downey L, Back AL, et al. Effect of a patient and clinician communication-priming intervention on patient-reported goals-of-care discussions between patients with serious illness and clinicians: a randomized clinical trial. JAMA Intern Med. 2018;178:930–940. doi: 10.1001/jamainternmed.2018.2317. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
