

Hemichorea Associated With Non-ketotic Hyperglycemia: A Case Report and Literature Review
- PMID: 32158423
- PMCID: PMC7052123
- DOI: 10.3389/fneur.2020.00096
Hemichorea Associated With Non-ketotic Hyperglycemia: A Case Report and Literature Review
Abstract
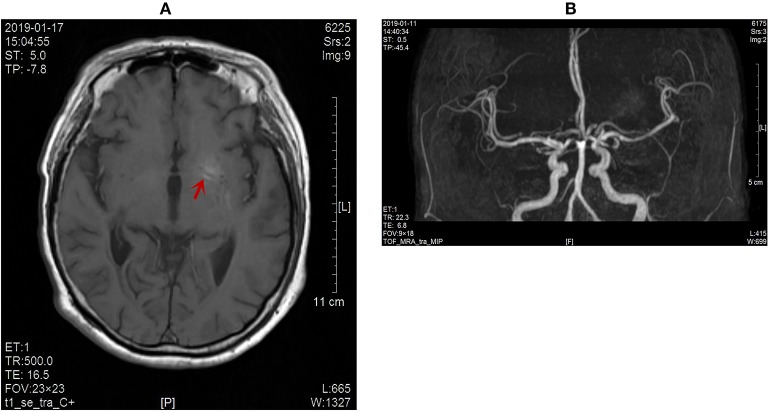
Objective: To explore the clinical manifestation, diagnosis, therapy, and mechanism of hemichorea associated with non-ketotic hyperglycemia (HC-NH) so as to enhance awareness and avoid misdiagnosis or missed diagnosis of the disease. Methods: A case of HC-NH was reported and reviewed in terms of the clinical features, diagnosis and treatment. Results: Hemichorea associated with non-ketotic hyperglycemia is a rare complication of diabetes mellitus, which is commonly seen in elderly women with poorly-controlled diabetes. The condition is characterized by non-ketotic hyperglycemia, unilateral involuntary choreiform movements, and contralateral basal ganglia hyper-intensity by T1-weighted MR imaging or high density on CT scans. Blood glucose control is the basal treatment, in combination with dopamine receptor antagonists and benzodiazepine sedative, in controlling hemichorea. Conclusion: In clinical practice, the possibility of unilateral chorea should be considered for diabetic patients with poor blood glucose control.
Keywords: blood glucose; hemichorea; lentiform nucleus; magnetic resonance imaging; non-ketotic hyperglycemia.
Copyright © 2020 Zheng, Chen, Chen, Lin, Tang, Lin, Wu, Lin and Lin.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources