

Rhino-Orbital-Cerebral Mucormycosis: Battle with the Deadly Enemy
- PMID: 32158665
- PMCID: PMC7040141
- DOI: 10.1007/s12070-019-01774-z
Rhino-Orbital-Cerebral Mucormycosis: Battle with the Deadly Enemy
Abstract
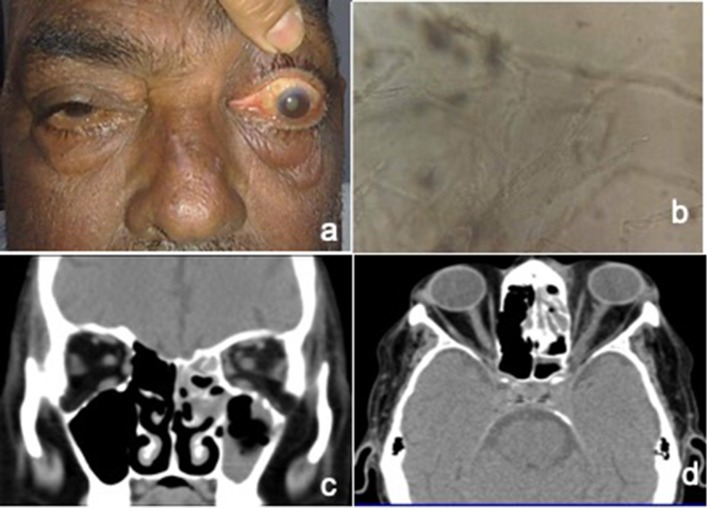
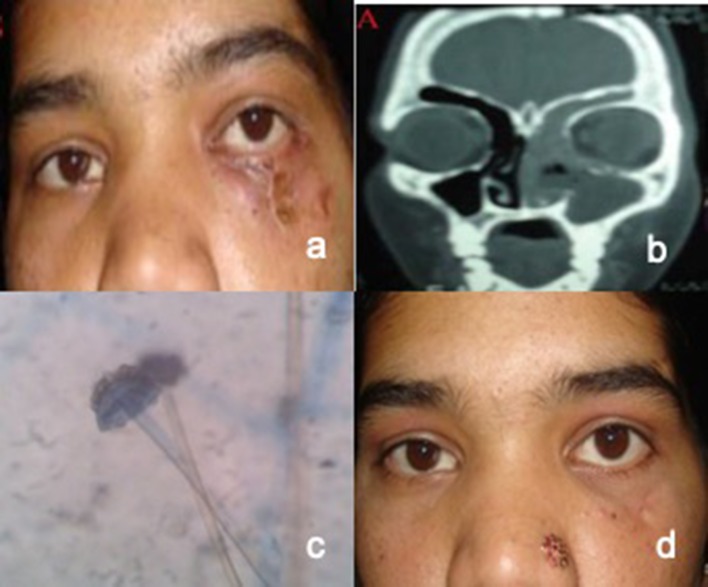
To study the clinical presentation and management outcomes in a series of patients with invasive rhino-orbital-cerebral mucormycosis presenting to a tertiary care center in central India. Medical records of eleven consecutive cases of invasive rhino-orbital-cerebral mucormycosis were reviewed. All clinically diagnosed cases, confirmed on microbiological examination were included. Their demographic data, clinical manifestations, underlying systemic conditions, microbiological and radiological reports, medical treatments, and surgical interventions were recorded and analyzed. There were nine male and two female patients with mean age of 46.8 years. Uncontrolled diabetes mellitus was noted in all patients. One patient had history of renal transplantation. The common presenting features were-ophthalmoplegia (73%), diminution of vision, (64%) proptosis (36%) and periorbital swelling (27%). CT scan/MRI revealed sino-orbital involvement in eight cases and rhino-orbital-cerebral involvement in three cases. Ethmoid sinus (100%) was the commonest paranasal sinus involved. KOH preparation and histopathology revealed broad aseptate filamentous fungi branching at right angles with tissue invasion. Culture on sabouraud's dextrose agar showed growth of mucor species. All patients received intravenous amphotericin B and had undergone radical debridement of involved sinuses. The mean duration of follow up was 13 months. All survived except three, who developed cerebral mucormycosis. Rhino-orbital-cerebral mucormycosis is a fetal fungal infection requiring multidisciplinary approach. Uncontrolled diabetes mellitus is the main predisposing factor. Early diagnosis, reversal of predisposing co-morbidities, aggressive medical and surgical management are vital in managing this highly aggressive disease.
Keywords: Diabetes mellitus; Mucormycosis; Ophthalmoplegia; Orbital apex syndrome; Orbital cellulitis.
© Association of Otolaryngologists of India 2019.
Conflict of interest statement
Conflicts of interestAll authors have declare that they have no conflict of interest.
Figures


References
LinkOut - more resources
Full Text Sources
Miscellaneous