

Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease
- PMID: 32158768
- PMCID: PMC7052117
- DOI: 10.3389/fcvm.2020.00022
Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease
Abstract
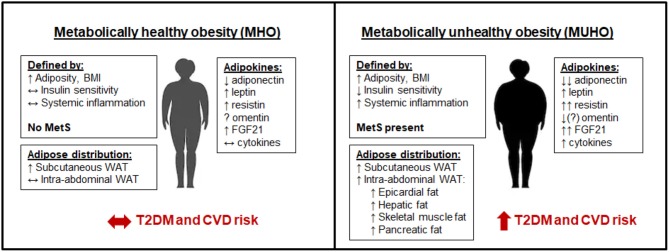
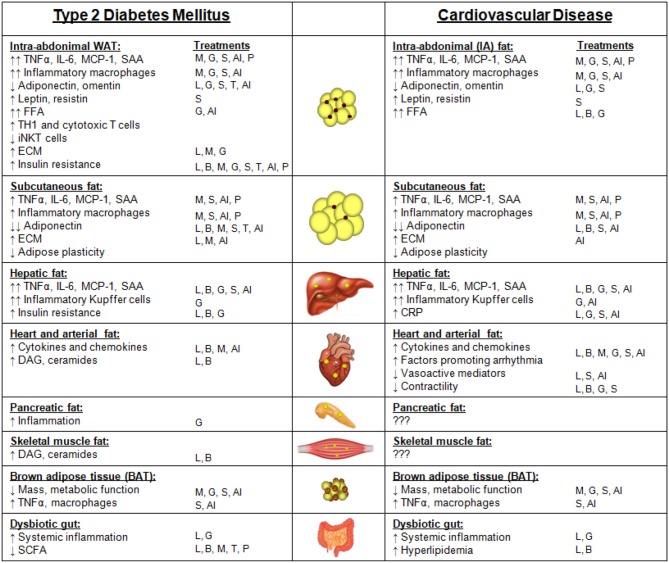
Adipose tissue plays essential roles in maintaining lipid and glucose homeostasis. To date several types of adipose tissue have been identified, namely white, brown, and beige, that reside in various specific anatomical locations throughout the body. The cellular composition, secretome, and location of these adipose depots define their function in health and metabolic disease. In obesity, adipose tissue becomes dysfunctional, promoting a pro-inflammatory, hyperlipidemic and insulin resistant environment that contributes to type 2 diabetes mellitus (T2DM). Concurrently, similar features that result from adipose tissue dysfunction also promote cardiovascular disease (CVD) by mechanisms that can be augmented by T2DM. The mechanisms by which dysfunctional adipose tissue simultaneously promote T2DM and CVD, focusing on adipose tissue depot-specific adipokines, inflammatory profiles, and metabolism, will be the focus of this review. The impact that various T2DM and CVD treatment strategies have on adipose tissue function and body weight also will be discussed.
Keywords: adipokines; beige adipose tissue; brown adipose tissue; insulin resistance; metabolic syndrome; subcutaneous white adipose tissue; visceral white adipose tissue.
Copyright © 2020 Chait and den Hartigh.
Figures
References
-
- Centers for Disease Control and Prevention (CDC) Prevalence of overweight and obesity among adults with diagnosed diabetes–United States, 1988-1994 and 1999-2002. MMWR Morb Mortal Wkly Rep. (2004) 53:1066–8. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources