

Tailored Three-Dimensionally Printed Triply Periodic Calcium Phosphate Implants: A Preclinical Study for Craniofacial Bone Repair
- PMID: 32158932
- PMCID: PMC7064275
- DOI: 10.1021/acsbiomaterials.9b01241
Tailored Three-Dimensionally Printed Triply Periodic Calcium Phosphate Implants: A Preclinical Study for Craniofacial Bone Repair
Erratum in
-
Correction to Tailored Three-Dimensionally Printed Triply Periodic Calcium Phosphate Implants: A Preclinical Study for Craniofacial Bone Repair.ACS Biomater Sci Eng. 2020 Mar 9;6(3):1821. doi: 10.1021/acsbiomaterials.0c00167. Epub 2020 Feb 20. ACS Biomater Sci Eng. 2020. PMID: 33455404 No abstract available.
Abstract
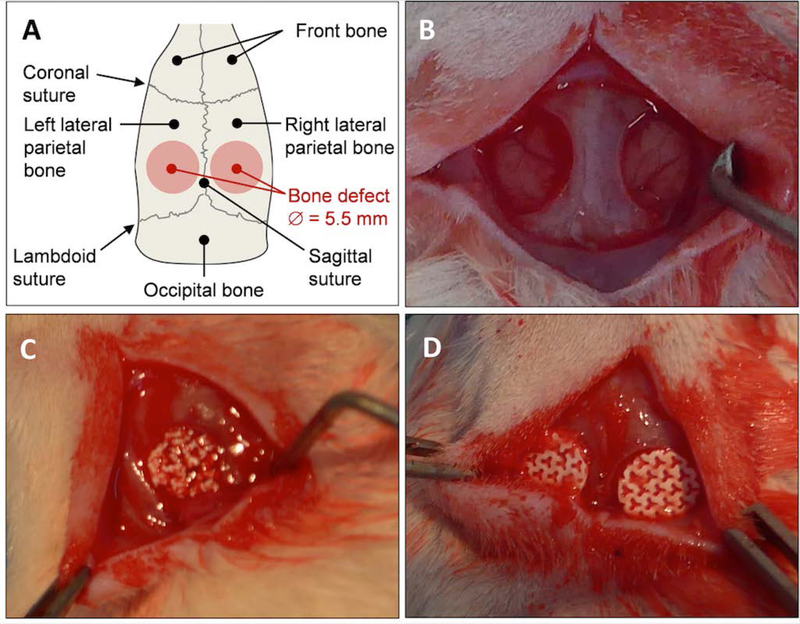
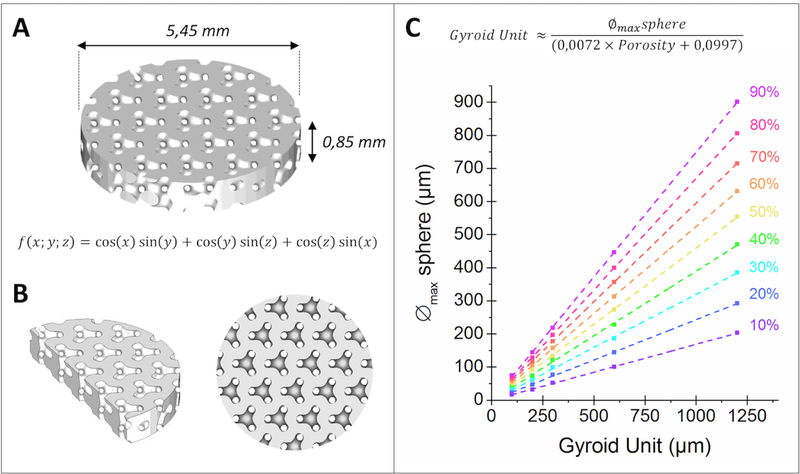
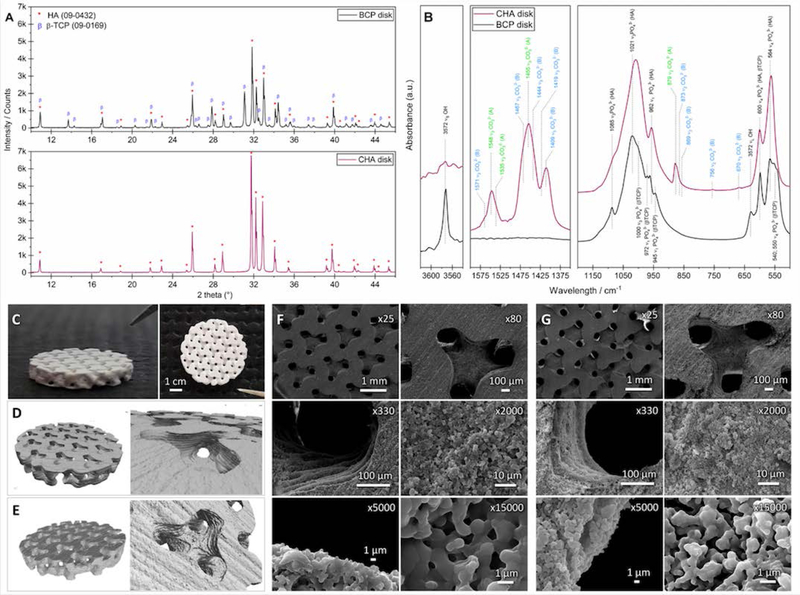
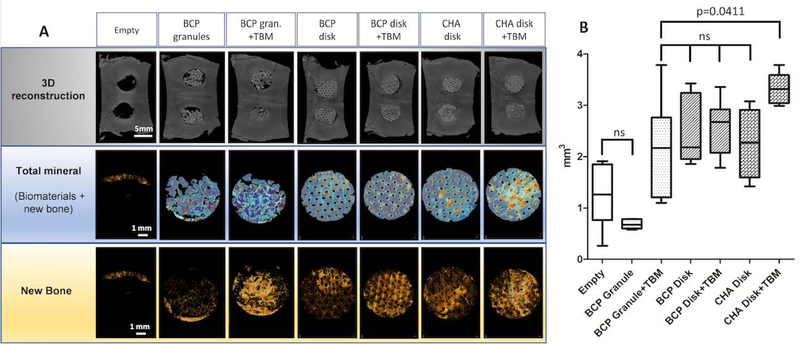
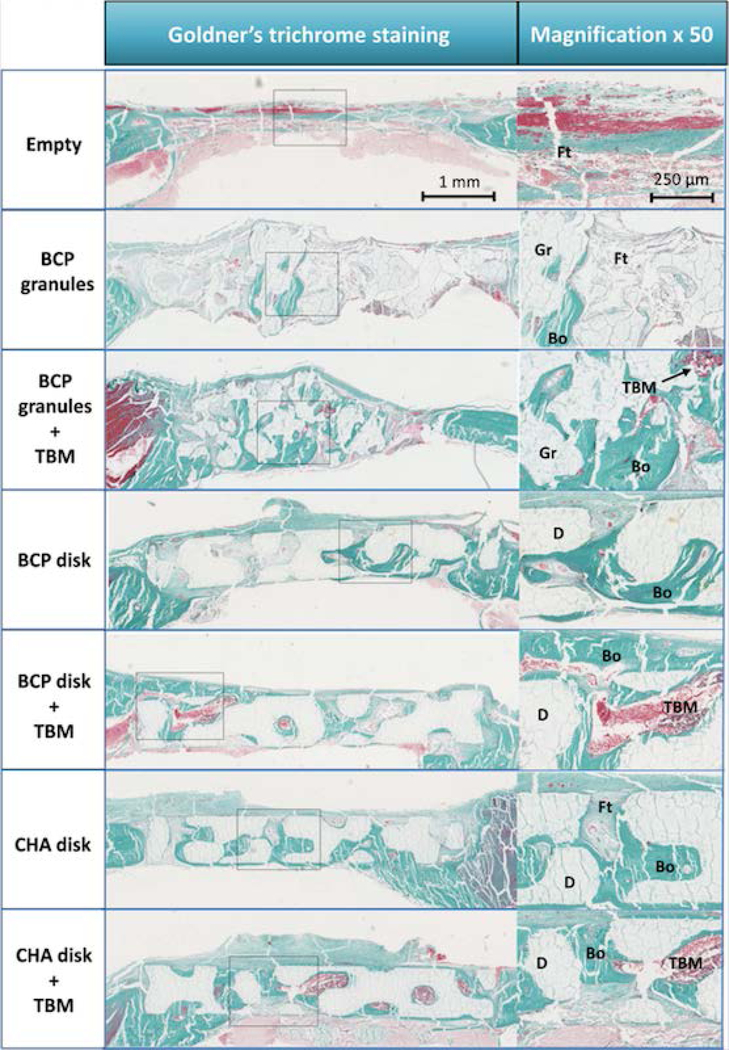
Finding alternative strategies for the regeneration of craniofacial bone defects (CSD), such as combining a synthetic ephemeral calcium phosphate (CaP) implant and/or active substances and cells, would contribute to solving this reconstructive roadblock. However, CaP's architectural features (i.e., architecture and composition) still need to be tailored, and the use of processed stem cells and synthetic active substances (e.g., recombinant human bone morphogenetic protein 2) drastically limits the clinical application of such approaches. Focusing on solutions that are directly transposable to the clinical setting, biphasic calcium phosphate (BCP) and carbonated hydroxyapatite (CHA) 3D-printed disks with a triply periodic minimal structure (TPMS) were implanted in calvarial critical-sized defects (rat model) with or without addition of total bone marrow (TBM). Bone regeneration within the defect was evaluated, and the outcomes were compared to a standard-care procedure based on BCP granules soaked with TBM (positive control). After 7 weeks, de novo bone formation was significantly greater in the CHA disks + TBM group than in the positive controls (3.33 mm3 and 2.15 mm3, respectively, P=0.04). These encouraging results indicate that both CHA and TPMS architectures are potentially advantageous in the repair of CSDs and that this one-step procedure warrants further clinical investigation.
Keywords: 3D printing; Bioceramics; Bone marrow; Bone tissue engineering; Calcium phosphates; Calvaria.
Conflict of interest statement
Conflicts of interest: None
Figures
References
-
- Honeybul S; Morrison DA; Ho KM; Lind CRP; Geelhoed E A Randomized Controlled Trial Comparing Autologous Cranioplasty with Custom-Made Titanium Cranioplasty. J. Neurosurg. 2017, 126 (1), 81–90. https://doi.org/10.317½015.12.JNS152004. - PubMed
-
- Dünisch P; Walter J; Sakr Y; Kalff R; Waschke A; Ewald C Risk Factors of Aseptic Bone Resorption: A Study after Autologous Bone Flap Reinsertion Due to Decompressive Craniotomy. J. Neurosurg. 2013, 118 (5), 1141–1147. https://doi.org/10.317½013.1.JNS12860. - PubMed
-
- Daculsi G; Baroth S; LeGeros R 20 Years of Biphasic Calcium Phosphate Bioceramics Development and Applications In Ceramic Engineering and Science Proceedings; Narayan R, Colombo P, Singh D, Salem J, Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2009; pp 45–58. 10.1002/9780470584354.ch5. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous