

Improving Electrocardiography Diagnostic Accuracy in Emergency Medical Services Personnel
- PMID: 32159079
- PMCID: PMC7063641
- DOI: 10.1016/j.cjco.2018.11.006
Improving Electrocardiography Diagnostic Accuracy in Emergency Medical Services Personnel
Abstract
Background: Accuracy of electrocardiogram (ECG) interpretation is important for identification of ST-elevation myocardial infarction (STEMI) by Emergency Medical Services (EMS) personnel who recognize STEMI in the field and activate the coronary catheterization laboratory. According to previous research, there is improvement in diagnosis of STEMIs for healthcare providers who read an average of > 20 ECGs per week. This study evaluated the effectiveness of online ECG modules on improving diagnostic accuracy.
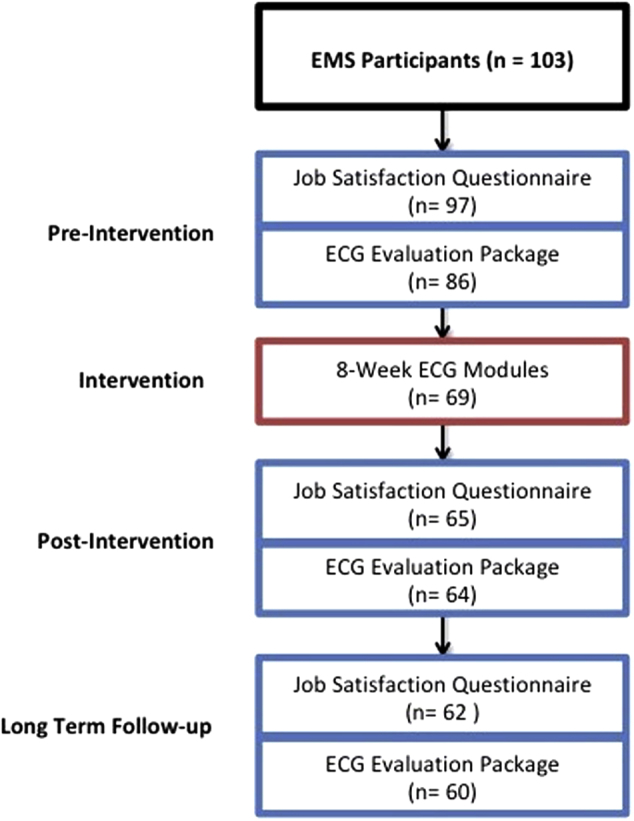
Methods: EMS personnel received 25 ECGs per week to interpret via an online program. Diagnostic accuracy was assessed for improvement via completion of an ECG evaluation package before and after the intervention. Job satisfaction data were collected to determine the impact of the educational initiative.
Results: A total of 64 participants completed the study. Overall, there was an improvement in ECG diagnostic accuracy from 50.8% to 61.2% (95% confidence interval [CI], 7.7-13.2; P < 0.0001). Specifically, there was significant improvement in the diagnosis of STEMI (8.5%; 95% CI, 4.9-12.3; P < 0.003) and supraventricular tachycardia (39.0%; 95% CI, 17.2-60.8; P < 0.008), with a trend toward improvement in all other diagnoses. These effects were sustained to 3 months (9.6%; 95% CI, 6.4-12.7; P < 0.0001). Improvement was seen regardless of employment experience and training. There was no significant impact on job satisfaction.
Conclusions: ECG exposure remains an important factor in improving the accuracy of ECG diagnosis in EMS personnel. Online education modules provide an easily accessible way of improving ECG interpretation with the opportunity for positive downstream effects on patient outcomes and resource use.
Introduction: L’interprétation de l’électrocardiogramme (ECG) doit être précise pour détecter l’infarctus du myocarde avec élévation du segment ST (STEMI) puisque le personnel des services médicaux d’urgence (SMU) doit reconnaître sur le terrain le STEMI et faire démarrer le processus vers le laboratoire de cathétérisme coronarien. Selon une étude antérieure, on note une amélioration dans le diagnostic du STEMI chez les prestataires de soins de santé qui lisent en moyenne > 20 ECG par semaine. La présente étude a permis d’évaluer l’efficacité des modules d’ECG en ligne en fonction de l’amélioration de la précision du diagnostic.
Méthodes: Le personnel des SMU recevait chaque semaine 25 ECG à interpréter au moyen d’un programme en ligne. On évaluait la précision du diagnostic en fonction de son amélioration en remplissant un module d’évaluation d’ECG avant et après l’intervention. Les données sur la satisfaction professionnelle étaient collectées pour déterminer les répercussions de l’initiative éducative.
Résultats: Un total de 64 participants ont complété l’étude. Dans l’ensemble, on a noté une amélioration de la précision du diagnostic à l’ECG, soit de 50,8 % à 61,2 % (intervalle de confiance [IC] à 95 %, 7,7-13,2; P < 0,0001). Notamment, on a noté une amélioration importante dans le diagnostic du STEMI (8,5 %; IC à 95 %, 4,9-12,3; P < 0,003) et de la tachycardie supraventriculaire (39,0 %; IC à 95 %, 17,2-60,8; P < 0,008), ainsi qu’une tendance à l’amélioration pour tous les autres diagnostics. Ces effets se sont maintenus jusqu’à 3 mois (9,6 %; IC à 95 %, 6,4-12,7; P < 0,0001). On a observé une amélioration, quelles que soient l’expérience professionnelle et la formation. Il n’y a eu aucune répercussion importante sur la satisfaction professionnelle.
Conclusions: L’exposition à l’ECG demeure un facteur important dans l’amélioration de la précision du diagnostic à l’ECG chez le personnel des SMU. Les modules éducatifs en ligne constituent des outils facilement accessibles pour améliorer l’interprétation de l’ECG en plus d’offrir la possibilité d’effets positifs en aval sur les résultats cliniques des patients et l’utilisation des ressources.
© 2018 Canadian Cardiovascular Society. Published by Elsevier Inc.
Figures




References
-
- O’Gara P.T., Kushner F.G., Ascheim D.D. 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:e362–e425. - PubMed
-
- Huitema A.A., Zhu T., Alemayehu M., Lavi S. Diagnostic accuracy of ST-segment elevation myocardial infarction by various healthcare providers. Int J Cardiol. 2014;177:825–829. - PubMed
-
- Sejersten M., Young D., Clemmensen P. Comparison of the ability of paramedics with that of cardiologists in diagnosing ST-segment elevation acute myocardial infarction in patients with acute chest pain. Am J Cardiol. 2002;90:995–998. - PubMed
-
- Rokos I.C., French W.J., Mattu A. Appropriate cardiac cath lab activation: optimizing electrocardiogram interpretation and clinical decision-making for acute ST-elevation myocardial infarction. Am Heart J. 2010;160:995–1003.e8. - PubMed
-
- Ornato J.P. The ST-segment–elevation myocardial infarction chain of survival. Circulation. 2007;116:6–9. - PubMed
LinkOut - more resources
Full Text Sources
