

Lead-Specific Features Predisposing to the Development of Tricuspid Regurgitation After Endocardial Lead Implantation
- PMID: 32159126
- PMCID: PMC7063659
- DOI: 10.1016/j.cjco.2019.10.002
Lead-Specific Features Predisposing to the Development of Tricuspid Regurgitation After Endocardial Lead Implantation
Abstract
Background: Endocardial lead in the right ventricle is recognized as a cause for tricuspid regurgitation (TR), but the mechanism remains elusive. We sought to evaluate lead-specific features on the development of TR after endocardial lead implantation.
Methods: This was a prospective single-center study. The patients underwent 2-dimensional echocardiograms before endocardial lead implantation and at follow-up visits at 4 to 6 weeks, 6 months, and 12 months. We assessed the position of the endocardial lead at the tricuspid annulus by 3-dimensional echocardiography, the tricuspid leaflet interference by the endocardial lead by both 2- and 3-dimensional echocardiography, and the degree of lead slack radiologically. Patient characteristics and lead-related factors were evaluated in the prediction of new or worse TR by univariable and multivariable analyses.
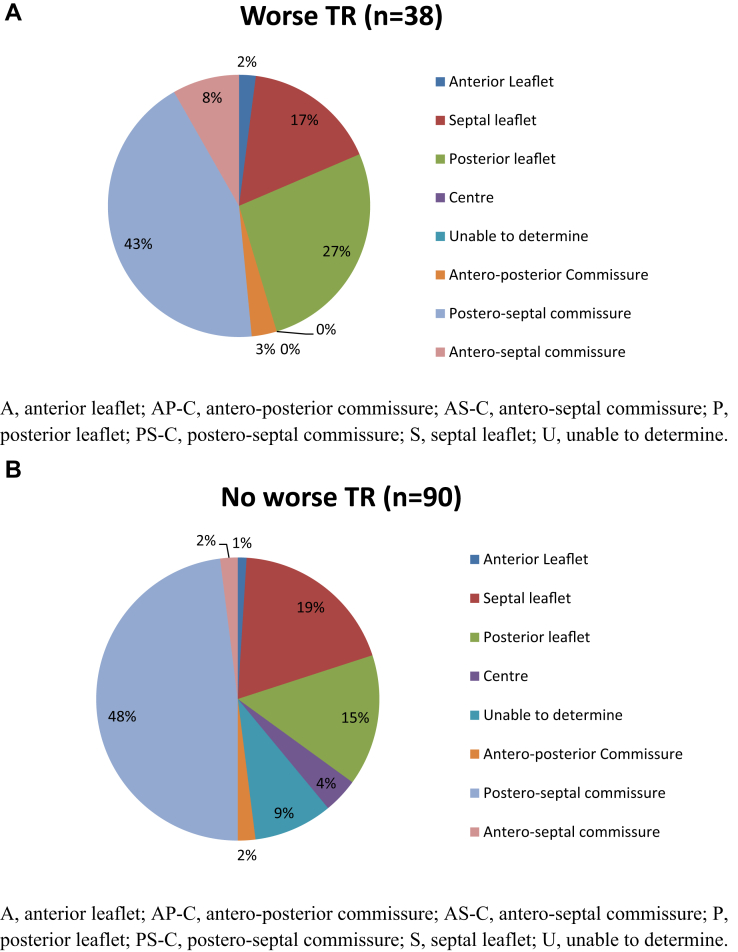
Results: New or increased TR was detected in 38 of 128 patients at the 12-month follow-up. The postero-septal commissure was the most common lead position, and tricuspid leaflet interference detected in 21 patients was associated with a noncommissural lead position. The implantation of an implantable cardioverter defibrillator lead was not associated with new TR compared with the implantation of a pacemaker lead. Tricuspid leaflet interference (P < 0.0001), but not lead position or lead slack, was the only lead-specific factor associated with the development of TR.
Conclusion: After right ventricle endocardial lead implantation, leaflet interference determined by echocardiography, but not the nature of the lead, the lead position at the tricuspid annulus, and the radiological lead slack, predicted TR development at 1 year postimplantation.
Contexte: Il est établi que la présence d’une sonde endocavitaire dans le ventricule droit est une cause de régurgitation tricuspide (RT), mais le mécanisme en cause n’est pas encore bien compris. Nous avons tenté d’évaluer la corrélation entre certaines caractéristiques des sondes et l’apparition d’une RT secondaire à l’implantation d’une sonde endocavitaire.
Méthodologie: Il s’agit d’une étude prospective menée dans un seul centre. Une échocardiographie bidimensionnelle a été réalisée avant la mise en place d’une sonde endocavitaire, ainsi qu’aux visites de suivi menées 4 à 6 semaines, 6 mois et 12 mois après l’intervention. Nous avons évalué la position de la sonde endocavitaire par rapport à l’anneau tricuspidien par échocardiographie tridimensionnelle, l’interférence de la sonde avec la valve tricuspide par échocardiographie bidimensionnelle et tridimensionnelle, et le degré de liberté de mouvement de la sonde par radiographie. Les caractéristiques des patients et les facteurs liés à la sonde ont été pris en compte dans la prédiction du risque de RT nouvelle ou d’aggravation d’une RT existante au moyen d’analyses univariées et multivariées.
Résultats: Une RT nouvelle ou aggravée a été détectée au suivi à 12 mois chez 38 des 128 patients. Dans la plupart des cas, la sonde se trouvait à la commissure postéroseptale; chez 21 patients, une interférence avec la valve tricuspide a été détectée alors que la sonde ne se trouvait pas à la commissure. La mise en place d'une sonde de défibrillateur implantable n’a pas été associée à l’apparition d’une RT, comparativement à l’implantation d'une sonde de stimulateur cardiaque. L’interférence avec la valve tricuspide (p < 0,0001) était le seul facteur lié à la sonde associé à l’apparition d’une RT; aucun lien n’a été établi avec la position et le degré de liberté de mouvement de la sonde.
Conclusion: Après la mise en place d’une sonde endocavitaire dans le ventricule droit, l’interférence avec la valve tricuspide établie par échocardiographie permettait de prédire l’apparition d’une RT dans l’année suivant la mise en place de la sonde sans égard au type de sonde, à sa position par rapport à l’anneau tricuspidien ou à la liberté de mouvement détectée par radiographie.
© 2019 Canadian Cardiovascular Society. Published by Elsevier Inc.
Figures

References
-
- Nachnani G.H., Gooch A.S., Hsu I. Systolic murmurs induced by pacemaker catheters. Arch Intern Med. 1969;124:202–205. - PubMed
-
- Chang J.D., Manning W.J., Ebrille E., Zimetbaum P.J. Tricuspid valve dysfunction following pacemaker or cardioverter-defibrillator implantation. J Am Coll Cardiol. 2017;69:2331–2341. - PubMed
-
- Al-Mohaissen M.A., Chan K.L. Prevalence and mechanism of tricuspid regurgitation following implantation of endocardial leads for pacemaker or cardioverter-defibrillator. J Am Soc Echocardiogr. 2012;25:245–252. - PubMed
-
- Lin G., Nishimura R.A., Connolly H.M. Severe symptomatic tricuspid valve regurgitation due to permanent pacemaker or implantable cardioverter-defibrillator leads. J Am Coll Cardiol. 2005;45:1672–1675. - PubMed
-
- Pfannmueller B., Hirnie G., Seegurger J. Tricuspid valve repair in the presence of a permanent ventricular pacemaker lead. Eur J Cardiothorac Surg. 2011;39:657–661. - PubMed
LinkOut - more resources
Full Text Sources
