

Association of Functional, Cognitive, and Psychological Measures With 1-Year Mortality in Patients Undergoing Major Surgery
- PMID: 32159753
- PMCID: PMC7066523
- DOI: 10.1001/jamasurg.2020.0091
Association of Functional, Cognitive, and Psychological Measures With 1-Year Mortality in Patients Undergoing Major Surgery
Abstract
Importance: More older adults are undergoing major surgery despite the greater risk of postoperative mortality. Although measures, such as functional, cognitive, and psychological status, are known to be crucial components of health in older persons, they are not often used in assessing the risk of adverse postoperative outcomes in older adults.
Objective: To determine the association between measures of physical, cognitive, and psychological function and 1-year mortality in older adults after major surgery.
Design, setting, and participants: Retrospective analysis of a prospective cohort study of participants 66 years or older who were enrolled in the nationally representative Health and Retirement Study and underwent 1 of 3 types of major surgery.
Exposures: Major surgery, including abdominal aortic aneurysm repair, coronary artery bypass graft, and colectomy.
Main outcomes and measures: Our outcome was mortality within 1 year of major surgery. Our primary associated factors included functional, cognitive, and psychological factors: dependence in activities of daily living (ADL), dependence in instrumental ADL, inability to walk several blocks, cognitive status, and presence of depression. We adjusted for other demographic and clinical predictors.
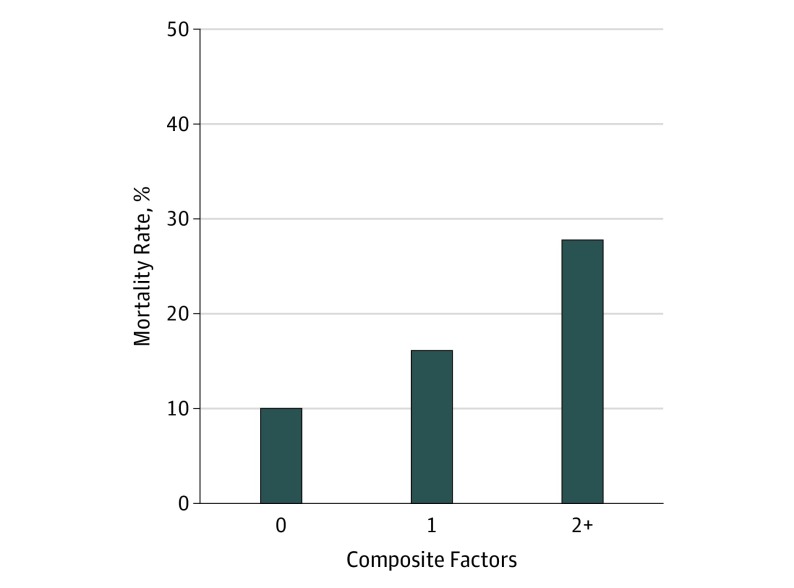
Results: Of 1341 participants, the mean (SD) participant age was 76 (6) years, 737 (55%) were women, 99 (7%) underwent abdominal aortic aneurysm repair, 686 (51%) coronary artery bypass graft, and 556 (42%) colectomy; 223 (17%) died within 1 year of their operation. After adjusting for age, comorbidity burden, surgical type, sex, race/ethnicity, wealth, income, and education, the following measures were significantly associated with 1-year mortality: more than 1 ADL dependence (29% vs 13%; adjusted hazard ratio [aHR], 2.76; P = .001), more than 1 instrumental ADL dependence (21% vs 14%; aHR, 1.32; P = .05), the inability to walk several blocks (17% vs 11%; aHR, 1.64; P = .01), dementia (21% vs 12%; aHR, 1.91; P = .03), and depression (19% vs 12%; aHR, 1.72; P = .01). The risk of 1-year mortality increased within the increasing risk factors present (0 factors: 10.0%; 1 factor: 16.2%; 2 factors: 27.8%).
Conclusions and relevance: In this older adult cohort, 223 participants (17%) who underwent major surgery died within 1 year and poor function, cognition, and psychological well-being were significantly associated with mortality. Measures in function, cognition, and psychological well-being need to be incorporated into the preoperative assessment to enhance surgical decision-making and patient counseling.
Conflict of interest statement
Figures
Comment in
-
Reframing Surgical Risk Using Geriatric Assessment Measures.JAMA Surg. 2020 May 1;155(5):418-419. doi: 10.1001/jamasurg.2020.0092. JAMA Surg. 2020. PMID: 32159739 No abstract available.
References
-
- Shahian DM, O’Brien SM, Sheng S, et al. . Predictors of long-term survival after coronary artery bypass grafting surgery: results from the Society of Thoracic Surgeons Adult Cardiac Surgery Database (the ASCERT study). Circulation. 2012;125(12):1491-1500. doi:10.1161/CIRCULATIONAHA.111.066902 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
