

Mid-trimester cervical length not associated with HIV status among pregnant women in Botswana
- PMID: 32160214
- PMCID: PMC7065819
- DOI: 10.1371/journal.pone.0229500
Mid-trimester cervical length not associated with HIV status among pregnant women in Botswana
Abstract
Objective: HIV-infected women on antiretroviral therapy have a higher risk of preterm birth than HIV-uninfected women in Botswana. To better understand the mechanism for preterm birth among HIV-infected women, we evaluated whether mid-trimester cervical length differed by HIV status as cervical shortening is associated with an increased risk for preterm birth.
Methods: We conducted a prospective cohort study among pregnant women receiving care at the Scottish Livingstone Hospital in Molepolole, Botswana. Consecutive women referred for routine obstetrical ultrasound were consented and enrolled if between 22w0d and 24w6d by ultrasound biometry. Blinded to maternal HIV status, an obstetrician measured transvaginal cervical length using standardized criteria. Cervical length, as well as the proportion of women with a short cervix (<25mm), were compared among HIV-infected and HIV-uninfected women. The acceptability of transvaginal ultrasound was also evaluated.
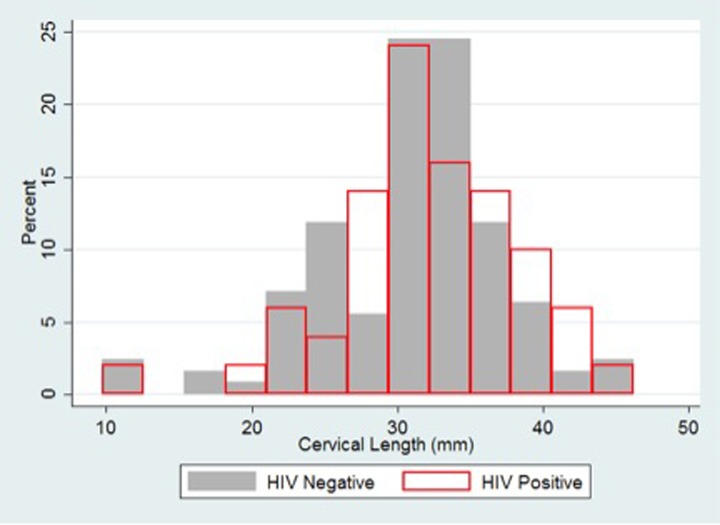
Results: Between April 2016 and April 2017, 853 women presenting for obstetric ultrasound were screened, 187 (22%) met eligibility criteria, and 179 (96%) were enrolled. Of those enrolled, 50 (28%) were HIV-infected (86% on antiretroviral therapy), 127 (71%) were HIV-uninfected, and 2 (1%) had unknown HIV status. There was no significant difference in mean cervical length between HIV-infected and HIV-uninfected women (32mm vs 31mm, p = 0.21), or in the proportion with a short cervix (10% vs 14%, p = 0.44). Acceptability data was available for 115 women who underwent a transvaginal ultrasound exam. Of these, 112 of 115 (97%) women deemed the transvaginal scan acceptable.
Conclusions: The increased risk of preterm birth observed among HIV-infected women receiving antiretroviral therapy in Botswana is unlikely associated with mid-trimester cervical shortening. Further research is needed to understand the underlying mechanism for preterm birth among HIV-infected women.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Stiehm E. R. et al. Efficacy of zidovudine and human immunodeficiency virus (HIV) hyperimmune immunoglobulin for reducing perinatal HIV transmission from HIV-infected women with advanced disease: results of Pediatric AIDS Clinical Trials Group protocol 185. J. Infect. Dis. 179, 567–575 (1999). 10.1086/314637 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
