

Visual seizure annotation and automated seizure detection using behind-the-ear electroencephalographic channels
- PMID: 32160324
- PMCID: PMC7217054
- DOI: 10.1111/epi.16470
Visual seizure annotation and automated seizure detection using behind-the-ear electroencephalographic channels
Abstract
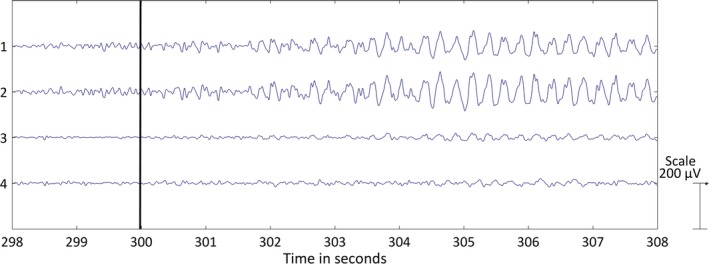
Objective: Seizure diaries kept by patients are unreliable. Automated electroencephalography (EEG)-based seizure detection systems are a useful support tool to objectively detect and register seizures during long-term video-EEG recording. However, this standard full scalp-EEG recording setup is of limited use outside the hospital, and a discreet, wearable device is needed for capturing seizures in the home setting. We are developing a wearable device that records EEG with behind-the-ear electrodes. In this study, we determined whether the recognition of ictal patterns using only behind-the-ear EEG channels is possible. Second, an automated seizure detection algorithm was developed using only those behind-the-ear EEG channels.
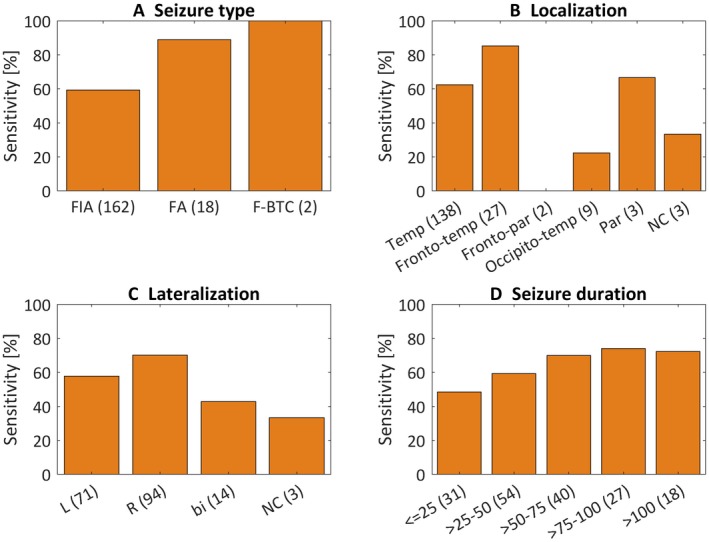
Methods: Fifty-four patients with a total of 182 seizures, mostly temporal lobe epilepsy (TLE), and 5284 hours of data, were recorded with a standard video-EEG at University Hospital Leuven. In addition, extra behind-the-ear EEG channels were recorded. First, a neurologist was asked to annotate behind-the-ear EEG segments containing selected seizure and nonseizure fragments. Second, a data-driven algorithm was developed using only behind-the-ear EEG. This algorithm was trained using data from other patients (patient-independent model) or from the same patient (patient-specific model).
Results: The visual recognition study resulted in 65.7% sensitivity and 94.4% specificity. By using those seizure annotations, the automated algorithm obtained 64.1% sensitivity and 2.8 false-positive detections (FPs)/24 hours with the patient-independent model. The patient-specific model achieved 69.1% sensitivity and 0.49 FPs/24 hours.
Significance: Visual recognition of ictal EEG patterns using only behind-the-ear EEG is possible in a significant number of patients with TLE. A patient-specific seizure detection algorithm using only behind-the-ear EEG was able to detect more seizures automatically than what patients typically report, with 0.49 FPs/24 hours. We conclude that a large number of refractory TLE patients can benefit from using this device.
Keywords: automated algorithms; behind-the-ear EEG; epilepsy; reduced electrode montage; seizure detection; wearable sensors.
© 2020 The Authors. Epilepsia published by Wiley Periodicals, Inc. on behalf of International League Against Epilepsy.
Conflict of interest statement
None of the authors has any conflict of interest to disclose. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Figures

References
-
- Forsgren L, Beghi E, Oun A, Sillanpää M. The epidemiology of epilepsy in Europe—a systematic review. Eur J Neurol. 2005;12:245–53. - PubMed
-
- French JA. Refractory epilepsy: clinical overview. Epilepsia. 2007;48:3–7. - PubMed
-
- Elger CE, Mormann F. Seizure prediction and documentation—two important problems. Lancet Neurol. 2013;12:531–2. - PubMed
-
- Blum DE, Eskola J, Bortz JJ, Fisher RS. Patient awareness of seizures. Neurology. 1996;47:260–4. - PubMed
-
- Fisher RS, Blum DE, DiVentura B, et al. Seizure diaries for clinical research and practice: limitations and future prospects. Epilepsy Behav. 2012;24:304–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
