

Clinicopathologic predictors of renal outcomes in light chain cast nephropathy: a multicenter retrospective study
- PMID: 32160635
- PMCID: PMC7243151
- DOI: 10.1182/blood.2019003807
Clinicopathologic predictors of renal outcomes in light chain cast nephropathy: a multicenter retrospective study
Abstract
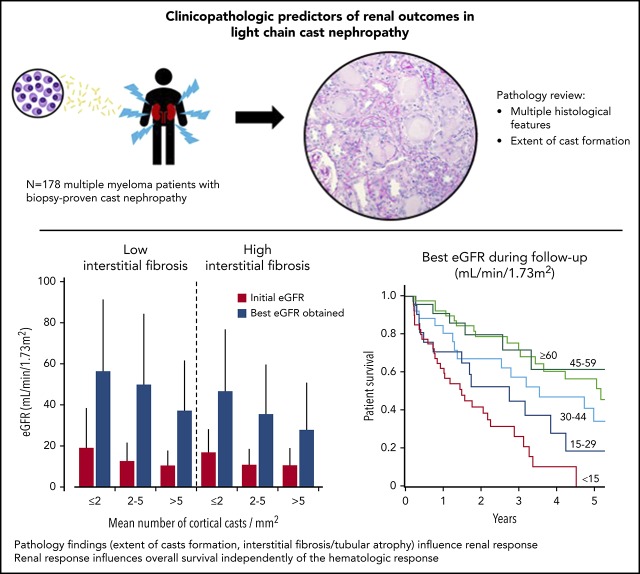
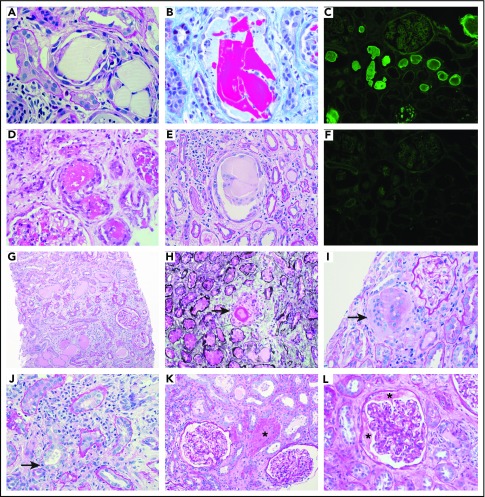
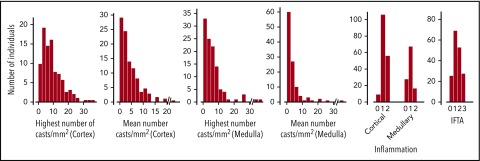
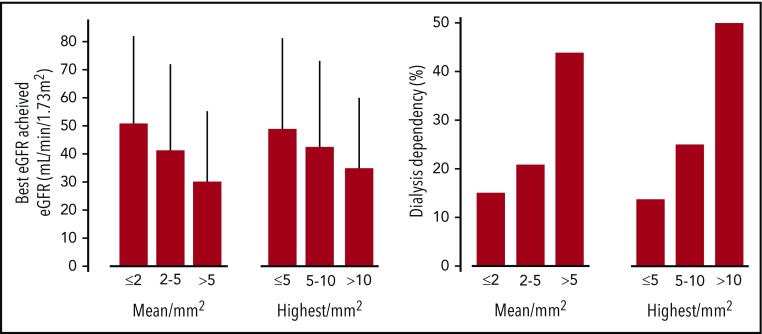
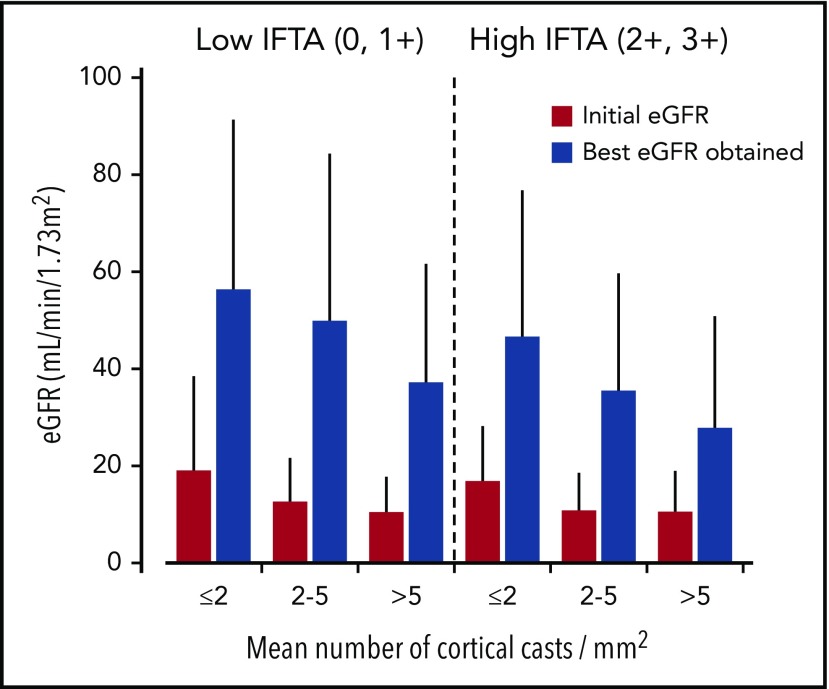
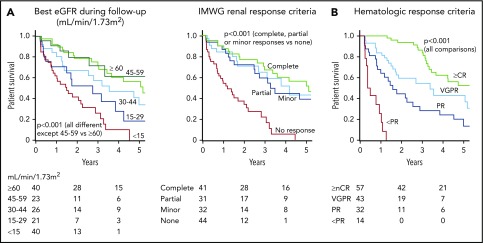
Light chain cast nephropathy (LCCN) in multiple myeloma often leads to severe and poorly reversible acute kidney injury. Severe renal impairment influences the allocation of chemotherapy and its tolerability; it also affects patient survival. Whether renal biopsy findings add to the clinical assessment in predicting renal and patient outcomes in LCCN is uncertain. We retrospectively reviewed clinical presentation, chemotherapy regimens, hematologic response, and renal and patient outcomes in 178 patients with biopsy-proven LCCN from 10 centers in Europe and North America. A detailed pathology review, including assessment of the extent of cast formation, was performed to study correlations with initial presentation and outcomes. Patients presented with a mean estimated glomerular filtration rate (eGFR) of 13 ± 11 mL/min/1.73 m2, and 82% had stage 3 acute kidney injury. The mean number of casts was 3.2/mm2 in the cortex. Tubulointerstitial lesions were frequent: acute tubular injury (94%), tubulitis (82%), tubular rupture (62%), giant cell reaction (60%), and cortical and medullary inflammation (95% and 75%, respectively). Medullary inflammation, giant cell reaction, and the extent of cast formation correlated with eGFR value at LCCN diagnosis. During a median follow-up of 22 months, mean eGFR increased to 43 ± 30 mL/min/1.73 m2. Age, β2-microglobulin, best hematologic response, number of cortical casts per square millimeter, and degree of interstitial fibrosis/tubular atrophy (IFTA) were independently associated with a higher eGFR during follow-up. This eGFR value correlated with overall survival, independently of the hematologic response. This study shows that extent of cast formation and IFTA in LCCN predicts the quality of renal response, which, in turn, is associated with overall survival.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- Kyle RA. Multiple myeloma: review of 869 cases. Mayo Clin Proc. 1975;50(1):29-40. - PubMed
-
- Knudsen LM, Hippe E, Hjorth M, Holmberg E, Westin J; The Nordic Myeloma Study Group . Renal function in newly diagnosed multiple myeloma—a demographic study of 1353 patients. Eur J Haematol. 1994;53(4):207-212. - PubMed
-
- Bladé J, Fernández-Llama P, Bosch F, et al. Renal failure in multiple myeloma: presenting features and predictors of outcome in 94 patients from a single institution. Arch Intern Med. 1998;158(17):1889-1893. - PubMed
-
- Knudsen LM, Hjorth M, Hippe E; Nordic Myeloma Study Group . Renal failure in multiple myeloma: reversibility and impact on the prognosis. Eur J Haematol. 2000;65(3):175-181. - PubMed
-
- Nasr SH, Valeri AM, Sethi S, et al. Clinicopathologic correlations in multiple myeloma: a case series of 190 patients with kidney biopsies. Am J Kidney Dis. 2012;59(6):786-794. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
