

Distinct Symptom-Specific Treatment Targets for Circuit-Based Neuromodulation
- PMID: 32160765
- PMCID: PMC8396109
- DOI: 10.1176/appi.ajp.2019.19090915
Distinct Symptom-Specific Treatment Targets for Circuit-Based Neuromodulation
Abstract
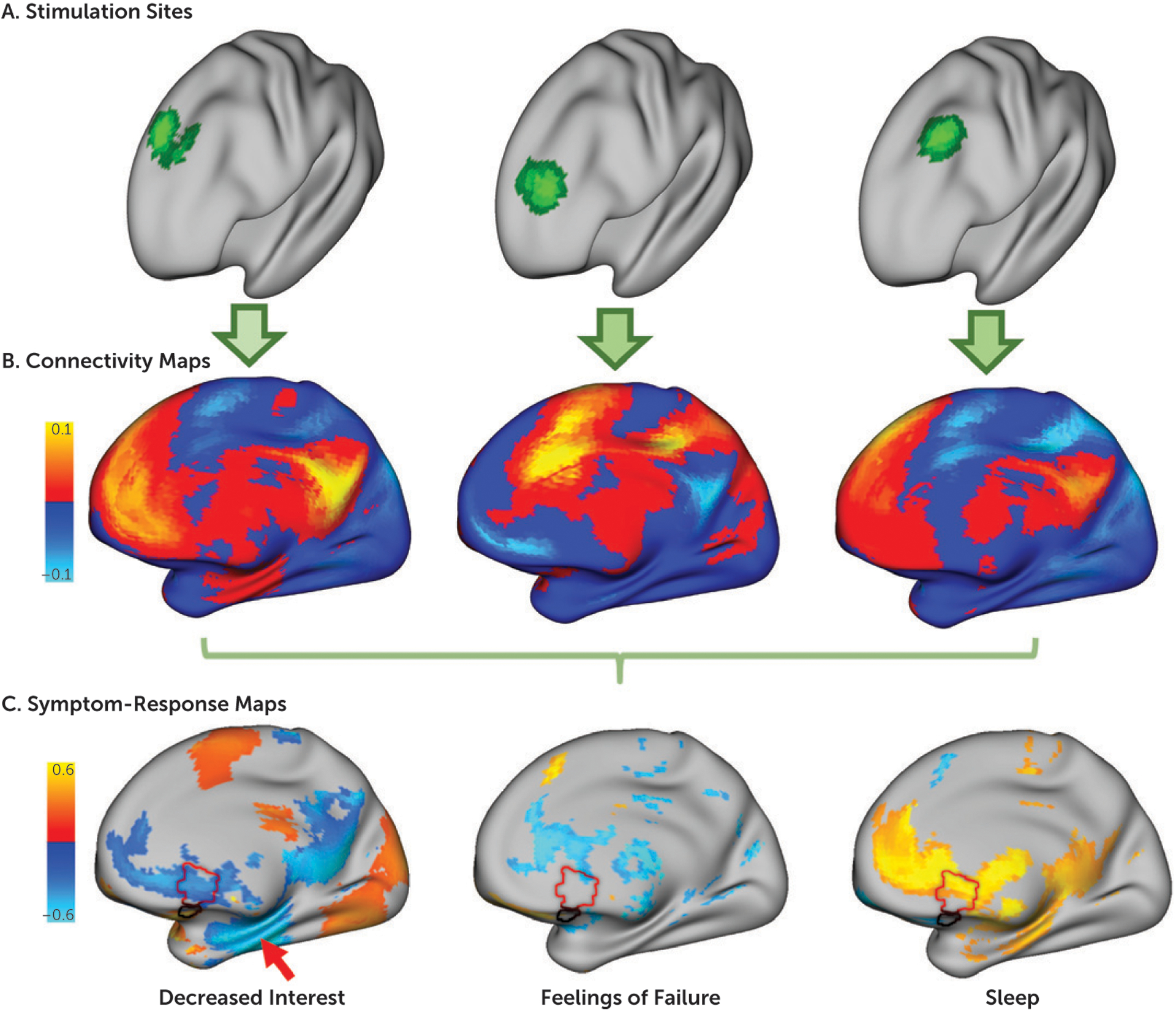
Objective: Treatment of different depression symptoms may require different brain stimulation targets with different underlying brain circuits. The authors sought to identify such targets, which could improve the efficacy of therapeutic brain stimulation and facilitate personalized therapy.
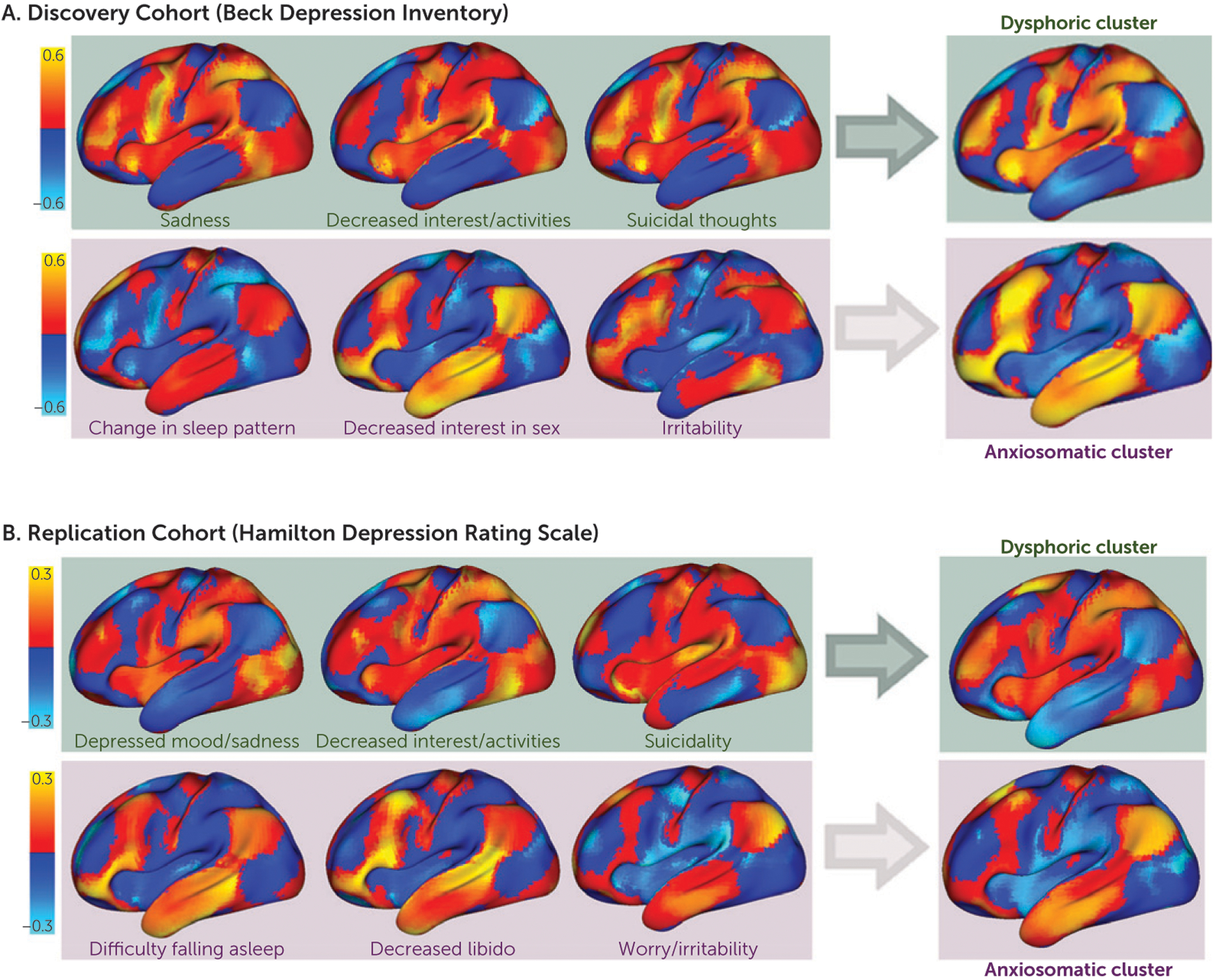
Methods: The authors retrospectively analyzed two independent cohorts of patients who received left prefrontal transcranial magnetic stimulation (TMS) for treatment of depression (discovery sample, N=30; active replication sample, N=81; sham replication sample, N=87). Each patient's TMS site was mapped to underlying brain circuits using functional connectivity MRI from a large connectome database (N=1,000). Circuits associated with improvement in each depression symptom were identified and then clustered based on similarity. The authors tested for reproducibility across data sets and whether symptom-specific targets derived from one data set could predict symptom improvement in the other independent cohort.
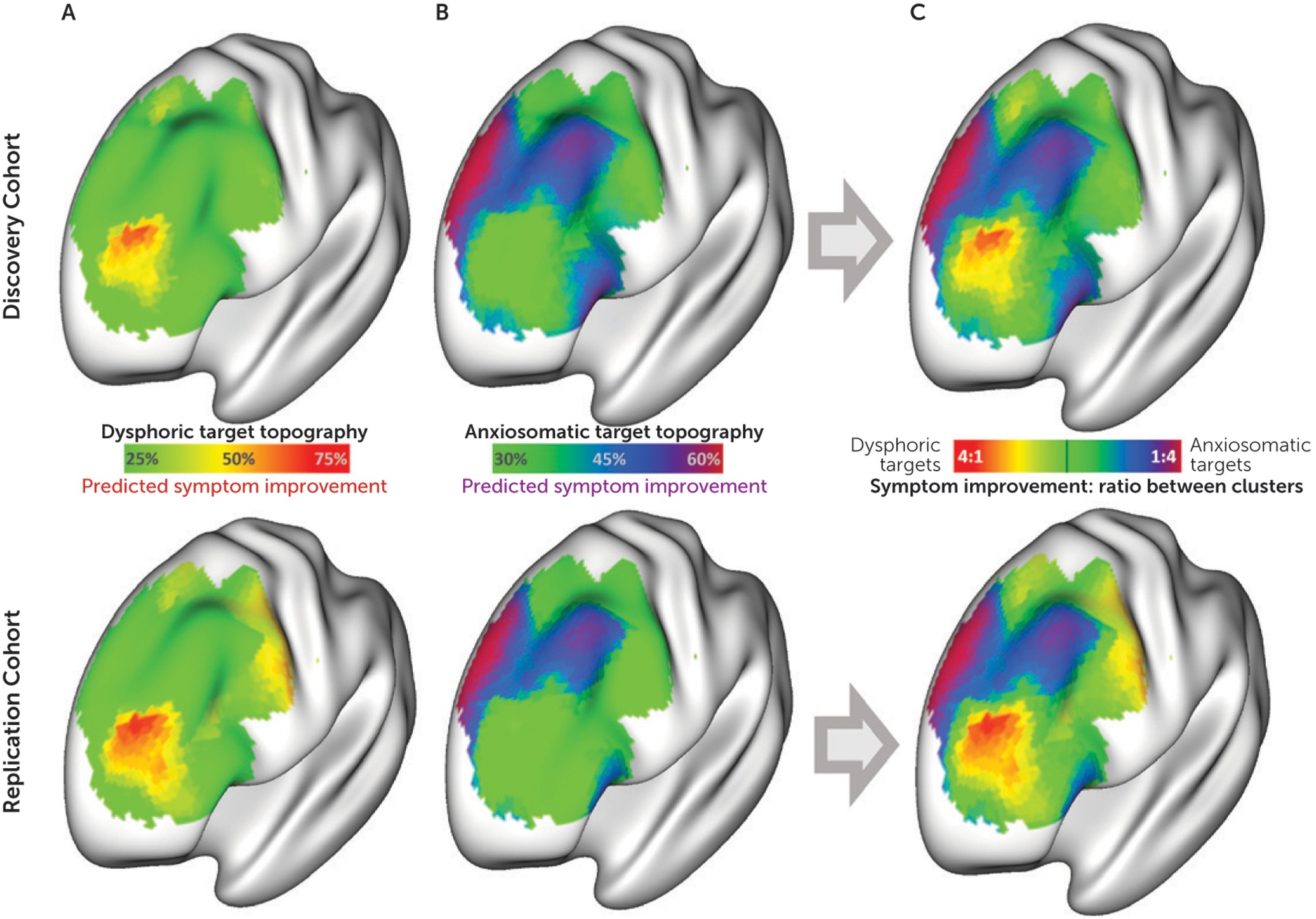
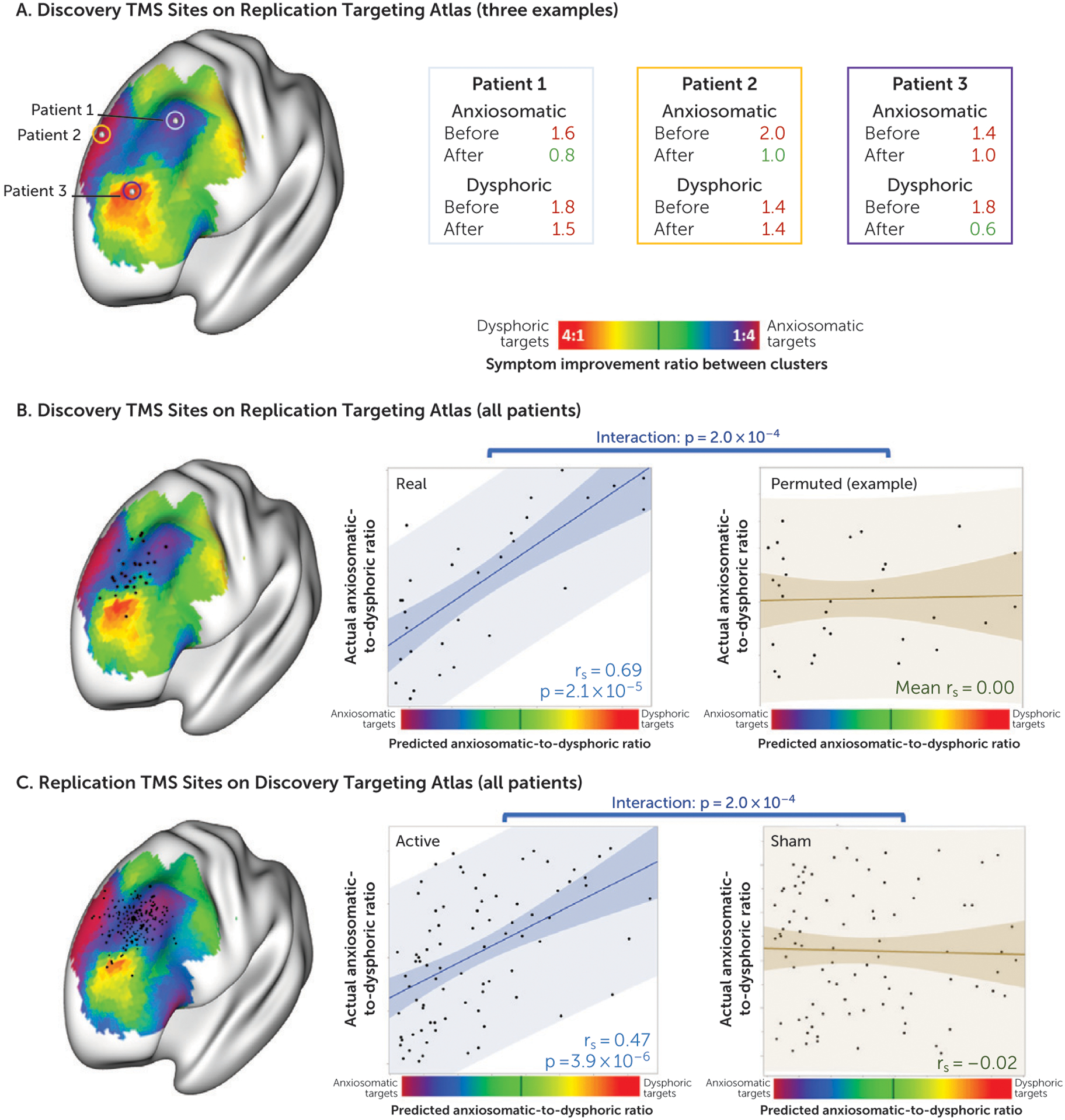
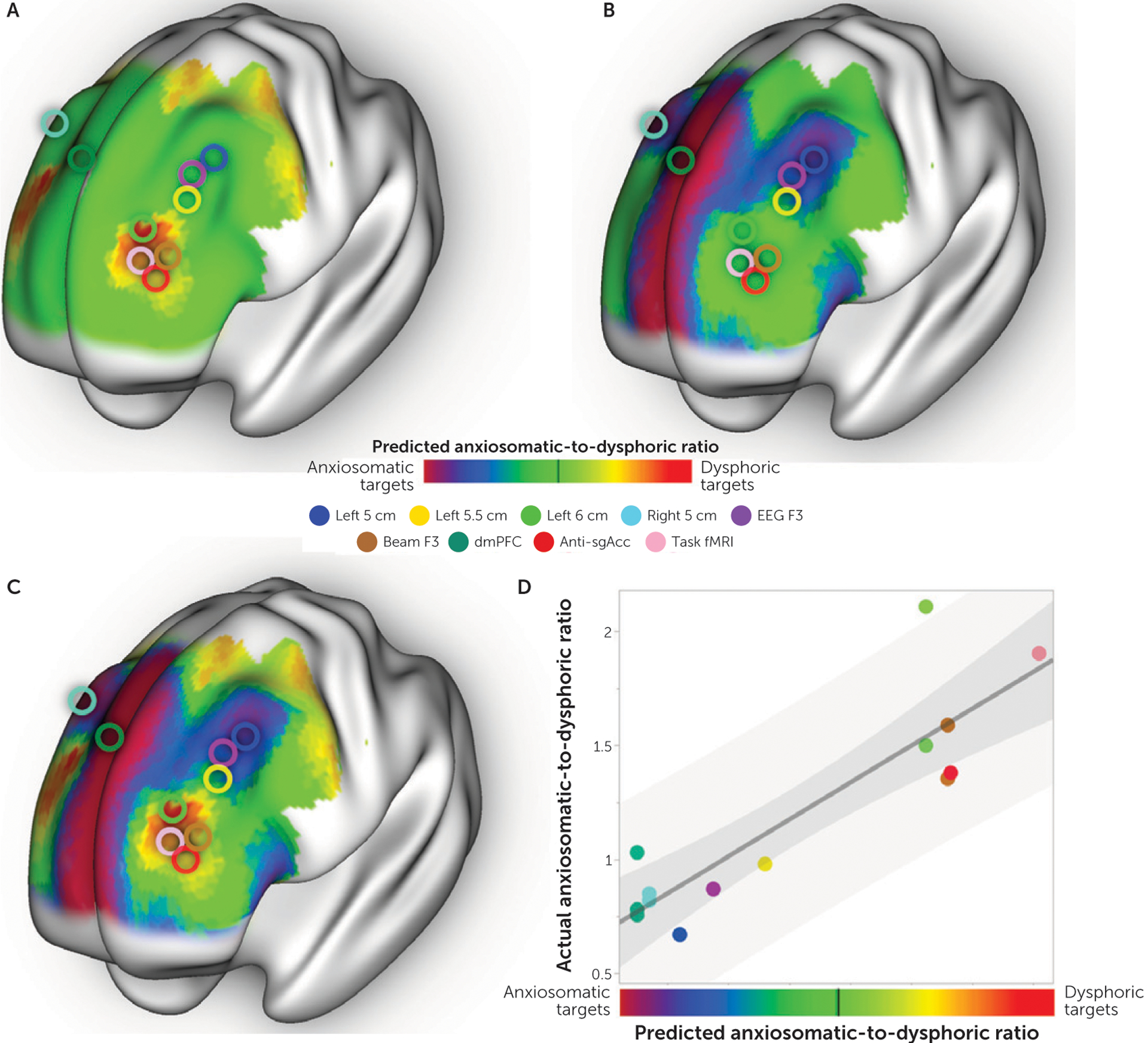
Results: The authors identified two distinct circuit targets effective for two discrete clusters of depressive symptoms. Dysphoric symptoms, such as sadness and anhedonia, responded best to stimulation of one circuit, while anxiety and somatic symptoms responded best to stimulation of a different circuit. These circuit maps were reproducible, predicted symptom improvement in independent patient cohorts, and were specific to active compared with sham stimulation. The maps predicted symptom improvement in an exploratory analysis of stimulation sites from 14 clinical TMS trials.
Conclusions: Distinct clusters of depressive symptoms responded better to different TMS targets across independent retrospective data sets. These symptom-specific targets can be prospectively tested in a randomized clinical trial. This data-driven approach for identifying symptom-specific targets may prove useful for other disorders and facilitate personalized neuromodulation therapy.
Keywords: Brain Imaging; Cognitive Neuroscience; Neuromodulation; Plasticity; TMS.
Figures
Comment in
-
Mapping Symptom Clusters to Circuits: Toward Personalizing TMS Targets to Improve Treatment Outcomes in Depression.Am J Psychiatry. 2020 May 1;177(5):373-375. doi: 10.1176/appi.ajp.2020.20030271. Am J Psychiatry. 2020. PMID: 32354264 No abstract available.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
