

Immunological risk stratification and tailored minimisation of immunosuppression in renal transplant recipients
- PMID: 32160893
- PMCID: PMC7065371
- DOI: 10.1186/s12882-020-01739-3
Immunological risk stratification and tailored minimisation of immunosuppression in renal transplant recipients
Abstract
Background: The efficacy and safety of minimisation of immunosuppression including early steroid withdrawal in kidney transplant recipients treated with Basiliximab induction remains unclear.
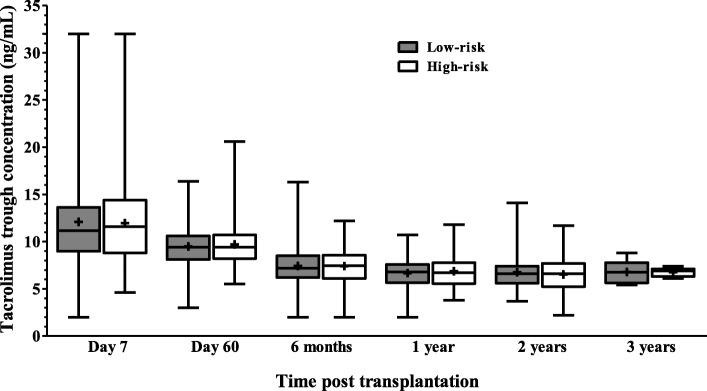
Methods: This retrospective cohort study reports the outcomes from 298 consecutive renal transplants performed since 1st July 2010-June 2013 treated with Basiliximab induction and early steroid withdrawal in low immunological risk patients using a simple immunological risk stratification and 3-month protocol biopsy to optimise therapy. The cohort comprised 225 low-risk patients (first transplant or HLA antibody calculated reaction frequency (CRF ≤50% with no donor specific HLA antibodies) who underwent basiliximab induction, steroid withdrawal on day 7 and maintenance with tacrolimus and mycophenolate mofetil (MMF), and 73 high-risk patients who received tacrolimus, MMF and prednisolone for the first 3 months followed by long term maintenance immunosuppression with tacrolimus and prednisolone. High-risk patients not undergoing 3-month protocol biopsy were continued on triple immunosuppression.
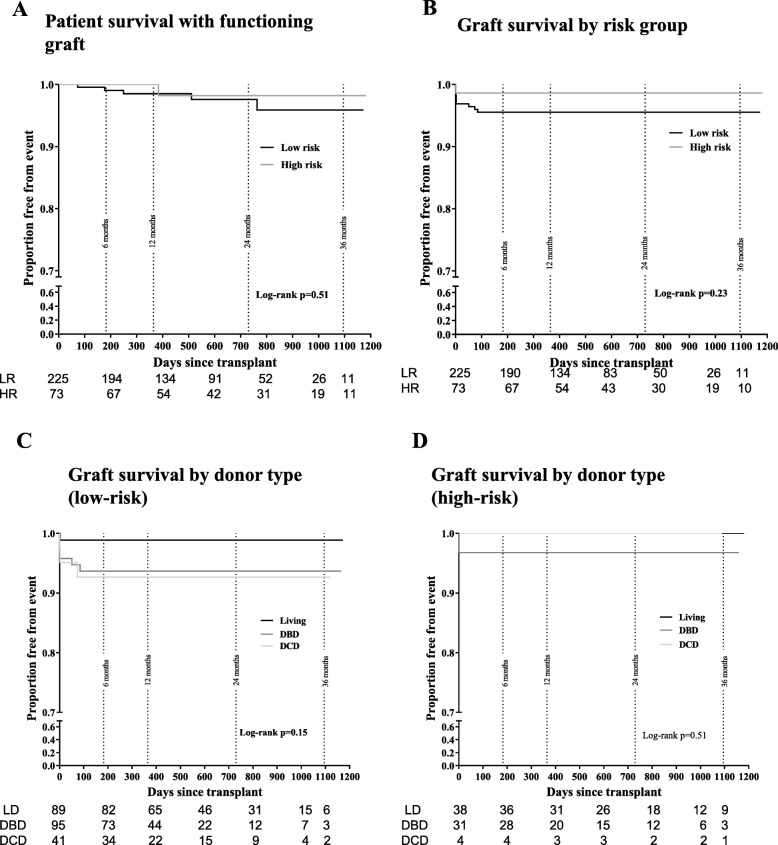
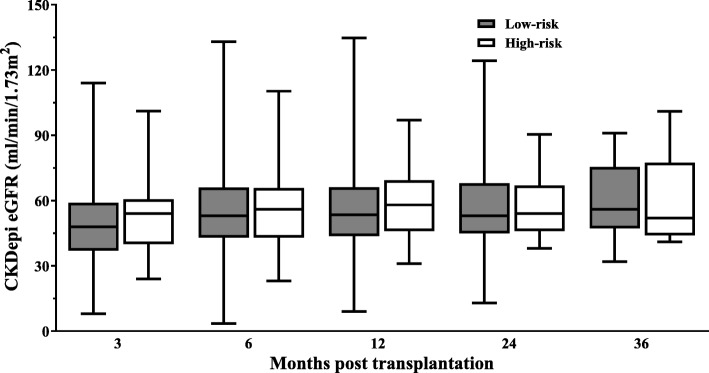
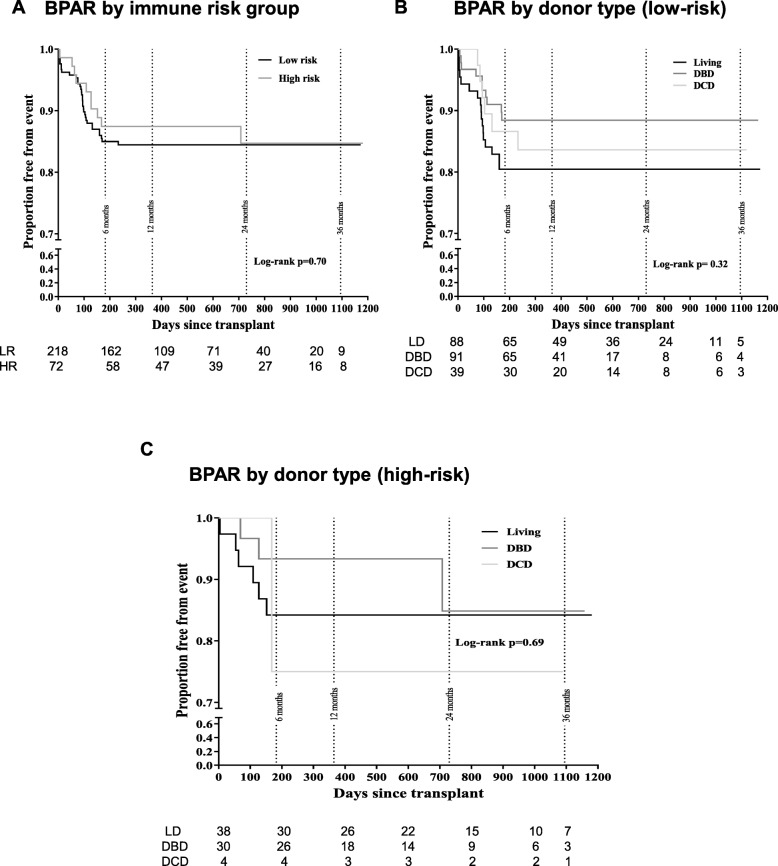
Results: Steroid withdrawal could be safely achieved in low immunological risk recipients with IL2 receptor antibody induction. The incidence of biopsy-proven acute rejection was 15.1% in the low-risk and 13.9% in the high-risk group (including sub-clinical rejection detected at protocol biopsy). One- year graft survival was 93.3% and patient survival 98.5% in the low-risk group, and 97.3 and 100% respectively in the high-risk group. Graft function was similar in each group at 1 year (mean eGFR 61.2 ± 23.4 mL/min low-risk and 64.6 ± 19.2 mL/min high-risk).
Conclusions: Immunosuppression regimen comprising basiliximab induction, tacrolimus, MMF and prednisolone with early steroid withdrawal in low risk patients and MMF withdrawal in high risk patients following a normal 3-month protocol biopsy is effective in limiting acute rejection episodes and produces excellent rates of patient survival, graft function and complications.
Keywords: Basiliximab; Corticosteroid-withdrawal; Mycophenolate mofetil; Renal transplantation; Tacrolimus.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Vincenti F, de Andres A, Becker T, et al. Interleukin-2 receptor antagonist induction in modern immunosuppression regimens for renal transplant recipients. Transplant international : official journal of the European Society for Organ Transplantation. 2006;19(6):446–457. doi: 10.1111/j.1432-2277.2006.00321.x. - DOI - PubMed
-
- Patlolla V, Zhong X, Reed GW, et al. Efficacy of anti-IL-2 receptor antibodies compared to no induction and to antilymphocyte antibodies in renal transplantation. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2007;7(7):1832–1842. doi: 10.1111/j.1600-6143.2007.01860.x. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
