

Left colon as a novel high-risk factor for postoperative recurrence of stage II colon cancer
- PMID: 32160919
- PMCID: PMC7066772
- DOI: 10.1186/s12957-020-01818-7
Left colon as a novel high-risk factor for postoperative recurrence of stage II colon cancer
Abstract
Background: It is not clear whether stage II colon and rectal cancer have the same risk factors for recurrence. Thus, the purpose of this study was to identify the risk factors for postoperative recurrence in stage II colorectal cancer.
Patients and methods: We retrospectively analyzed the data of 990 patients who had undergone radical surgery for stage II colorectal cancer. Patients' pathological features and characteristics including age, sex, family history, body mass index, tumor diameter, gross type of tumor, infiltration degree (T3/T4), tumor grade, perineural invasion, vascular invasion, lymphatic invasion, pathologic examination of lymph node number, and preoperative carcinoembryonic assay (CEA) level was compared between patients with and without recurrence. Finally, the prediction of the left and right colons was analyzed.
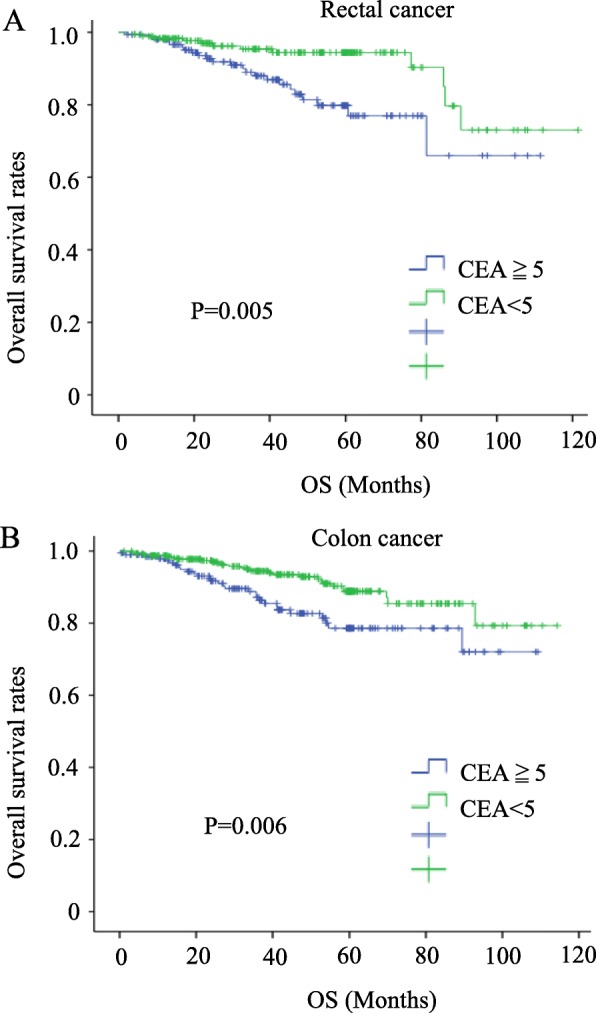
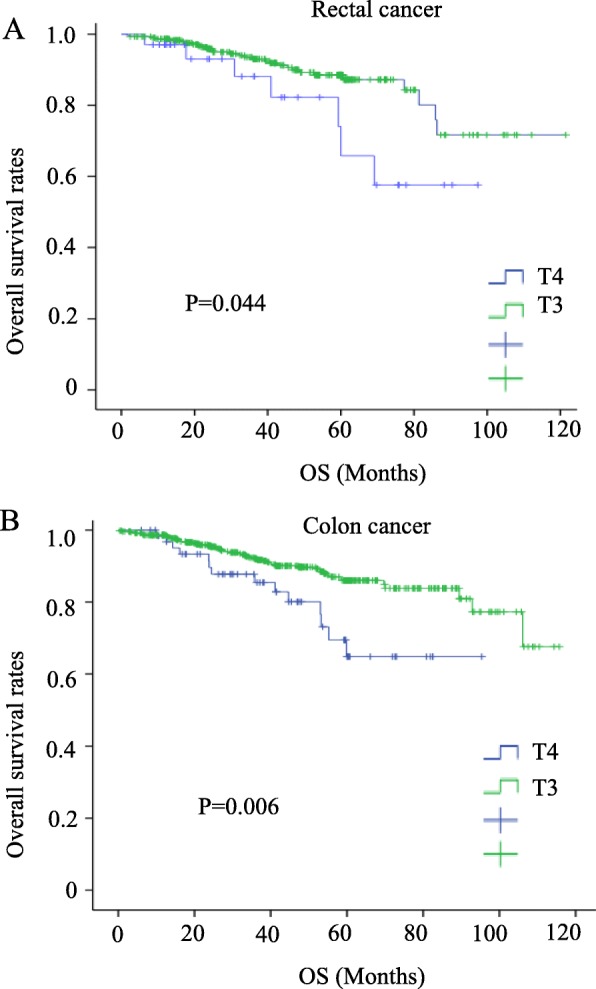
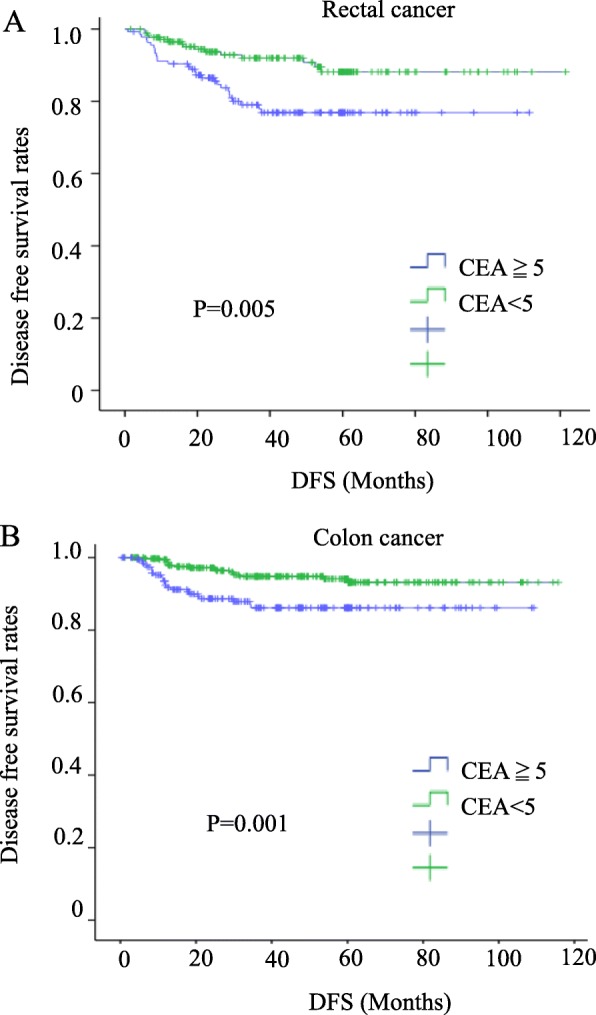
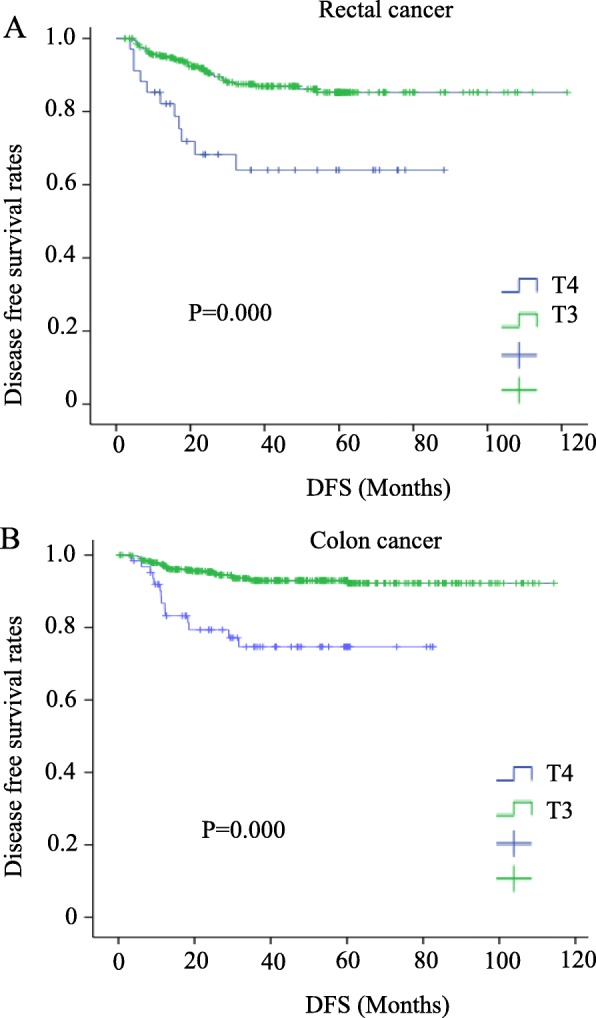
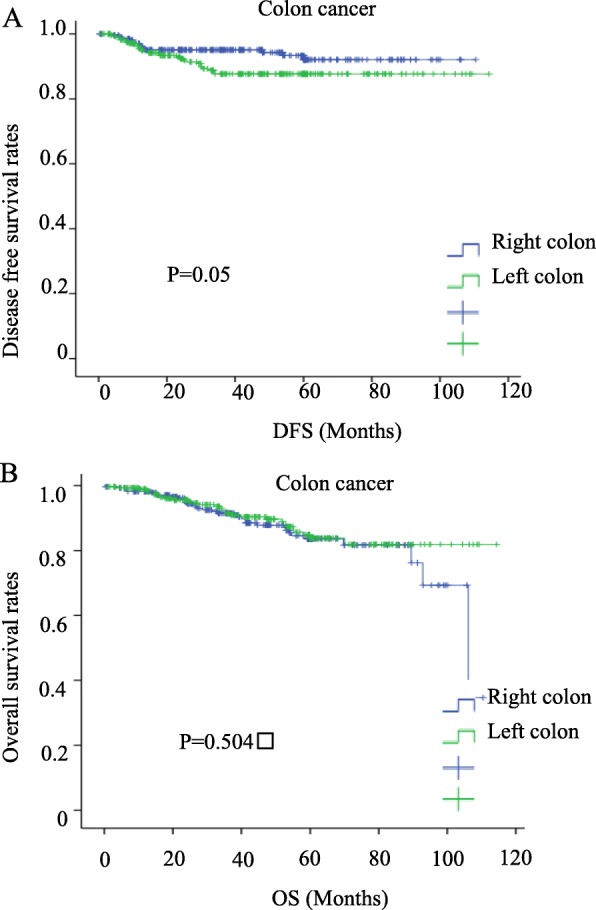
Results: The mean ages of the colon cancer and rectal cancer patients were 69.5 years and 66.4 years, respectively. In total, 508 (82.1%) and 285 (76.8%) patients were treated laparoscopically for colon cancer and rectal cancer, respectively, with median follow-up periods of 42.2 months and 41.8 months, respectively. Forty-four recurrences occurred in both the colon cancer (7.1%) and rectal cancer (11.9%) groups. The preoperative serum CEA level and T4 infiltration were significantly higher in recurrent colorectal cancer patients. The postoperative recurrence rate of left colon cancer (descending colon, sigmoid colon) was higher than that of right colon cancer (cecum, ascending colon, transverse colon) (OR 2.191, 95% CI 1.091-4.400, P = 0.027). In COX survival factor analysis of colon cancer, the left colon is one of the independent risk factors (risk ratio 5.377, 95% CI 0.216-0.88, P = 0.02). In disease-free survival (DFS), the left colon has a relatively poor prognosis (P = 0.05). However, in the COX analysis and prognosis analysis of OS, no difference was found between the left colon and the right colon.
Conclusion: Preoperative CEA and depth of infiltration (T4) are high-risk factors associated with recurrence and are prognostic factors in stage II colorectal cancer. Left colon is also a risk factor for postoperative recurrence of stage II colon cancer.
Keywords: Carcinoembryonic antigen; Colorectal cancer; Left colon cancer; Stage II.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018 68(6):394-424. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
