

Imported Malaria in Countries where Malaria Is Not Endemic: a Comparison of Semi-immune and Nonimmune Travelers
- PMID: 32161068
- PMCID: PMC7067581
- DOI: 10.1128/CMR.00104-19
Imported Malaria in Countries where Malaria Is Not Endemic: a Comparison of Semi-immune and Nonimmune Travelers
Abstract
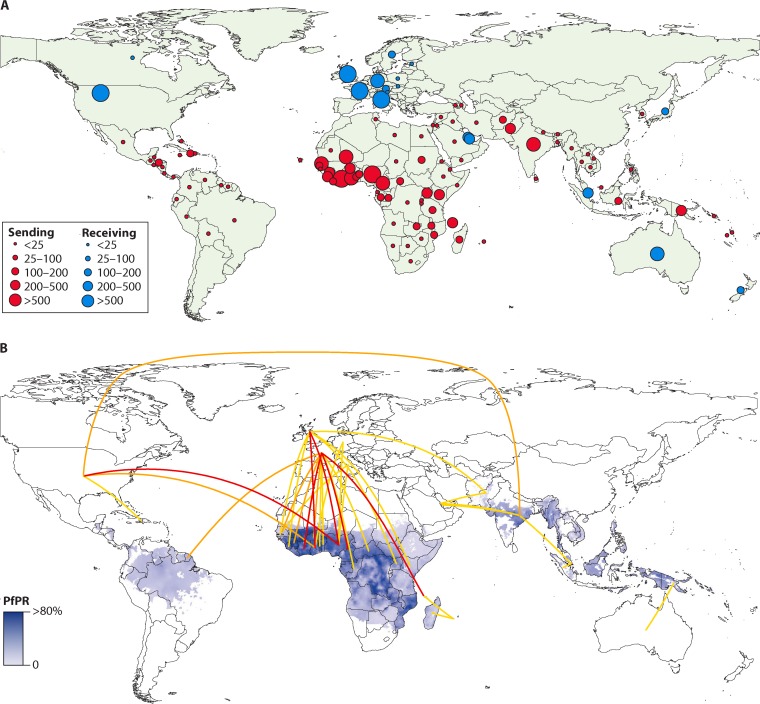
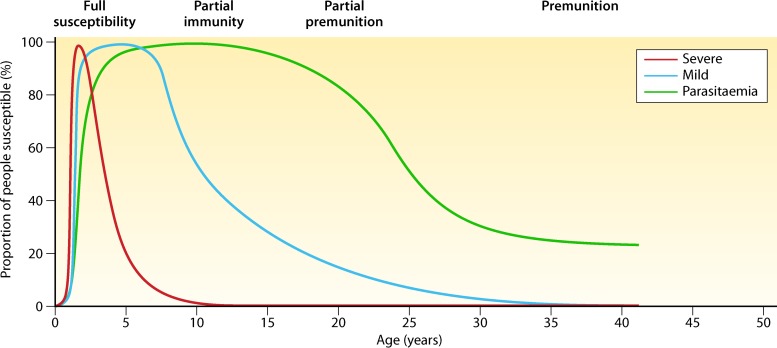
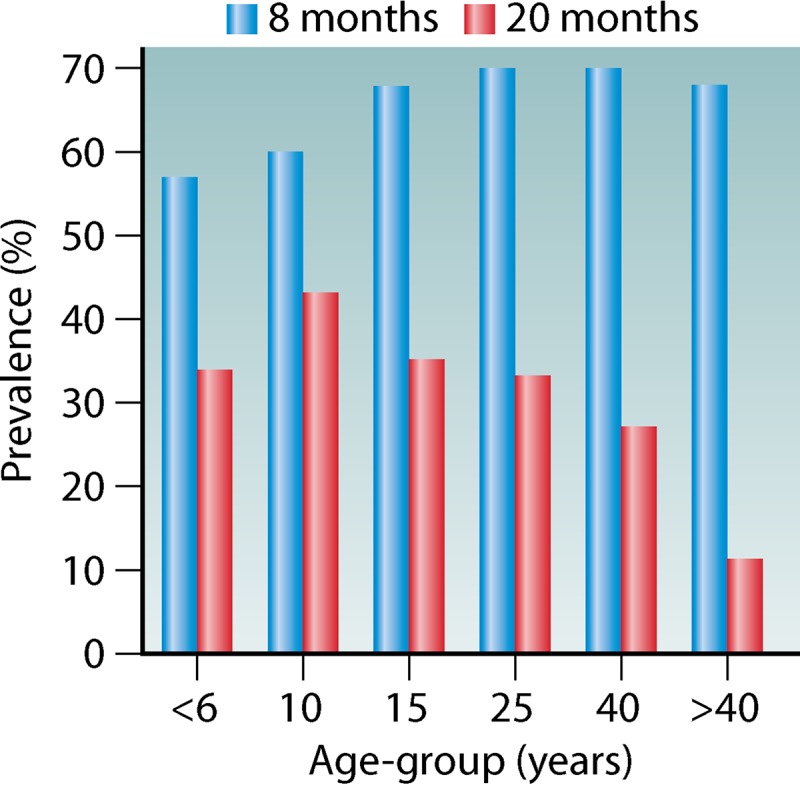
The continuous increase in long-distance travel and recent large migratory movements have changed the epidemiological characteristics of imported malaria in countries where malaria is not endemic (here termed non-malaria-endemic countries). While malaria was primarily imported to nonendemic countries by returning travelers, the proportion of immigrants from malaria-endemic regions and travelers visiting friends and relatives (VFRs) in malaria-endemic countries has continued to increase. VFRs and immigrants from malaria-endemic countries now make up the majority of malaria patients in many nonendemic countries. Importantly, this group is characterized by various degrees of semi-immunity to malaria, resulting from repeated exposure to infection and a gradual decline of protection as a result of prolonged residence in non-malaria-endemic regions. Most studies indicate an effect of naturally acquired immunity in VFRs, leading to differences in the parasitological features, clinical manifestation, and odds for severe malaria and clinical complications between immune VFRs and nonimmune returning travelers. There are no valid data indicating evidence for differing algorithms for chemoprophylaxis or antimalarial treatment in semi-immune versus nonimmune malaria patients. So far, no robust biomarkers exist that properly reflect anti-parasite or clinical immunity. Until they are found, researchers should rigorously stratify their study results using surrogate markers, such as duration of time spent outside a malaria-endemic country.
Keywords: Europe; VFR; clinical characteristics; diagnosis; imported; malaria; nonimmune; prophylaxis; semi-immune; treatment.
Copyright © 2020 American Society for Microbiology.
Figures
References
-
- World Health Organization. 2018. World malaria report 2018. World Health Organization, Geneva, Switzerland.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
