

The role of cellular senescence in ageing and endocrine disease
- PMID: 32161396
- PMCID: PMC7227781
- DOI: 10.1038/s41574-020-0335-y
The role of cellular senescence in ageing and endocrine disease
Abstract
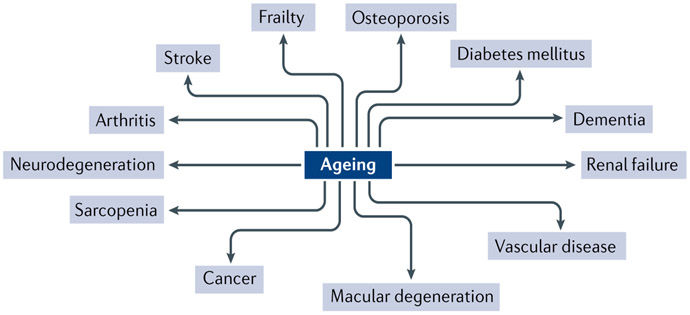
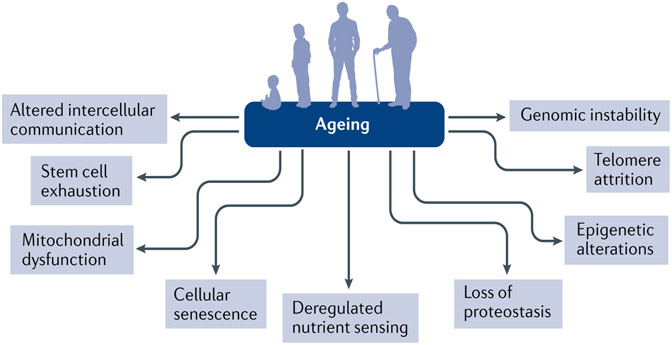
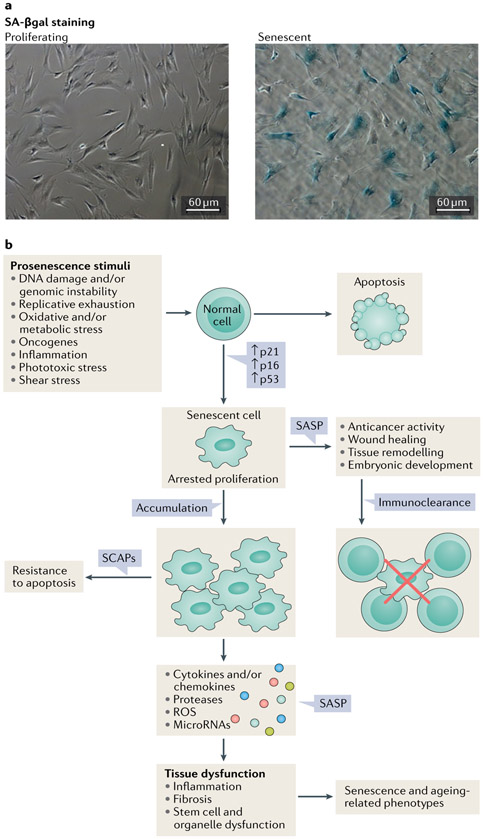
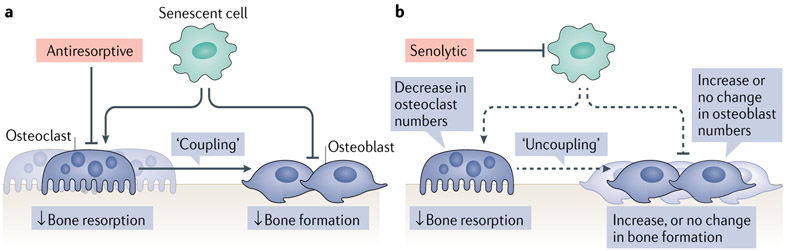
With the ageing of the global population, interest is growing in the 'geroscience hypothesis', which posits that manipulation of fundamental ageing mechanisms will delay (in parallel) the appearance or severity of multiple chronic, non-communicable diseases, as these diseases share the same underlying risk factor - namely, ageing. In this context, cellular senescence has received considerable attention as a potential target in preventing or treating multiple age-related diseases and increasing healthspan. Here we review mechanisms of cellular senescence and approaches to target this pathway therapeutically using 'senolytic' drugs that kill senescent cells or inhibitors of the senescence-associated secretory phenotype (SASP). Furthermore, we highlight the evidence that cellular senescence has a causative role in multiple diseases associated with ageing. Finally, we focus on the role of cellular senescence in a number of endocrine diseases, including osteoporosis, metabolic syndrome and type 2 diabetes mellitus, as well as other endocrine conditions. Although much remains to be done, considerable preclinical evidence is now leading to the initiation of proof-of-concept clinical trials using senolytics for several endocrine and non-endocrine diseases.
Conflict of interest statement
Competing interests
T.T. and J.L.K. have a financial interest related to this research. Patents on senolytic drugs are held by Mayo Clinic. Mayo Clinic has licensed patents on dasatinib and quercetin as senolytics to Unity Biotechnology. This research was reviewed by the Mayo Clinic Conflict of Interest Review Board and was conducted in compliance with Mayo Clinic conflict of interest policies. All other authors declare no competing interests.
Figures
References
-
- Levy HB Polypharmacy reduction strategies: tips on incorporating American Geriatrics Society Beers and Screening Tool of Older People’s Prescriptions criteria. Clin. Geriatr. Med 33, 177–187 (2017). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
