

Predicting the risk of depression among adolescents in Nepal using a model developed in Brazil: the IDEA Project
- PMID: 32162056
- PMCID: PMC7486232
- DOI: 10.1007/s00787-020-01505-8
Predicting the risk of depression among adolescents in Nepal using a model developed in Brazil: the IDEA Project
Abstract
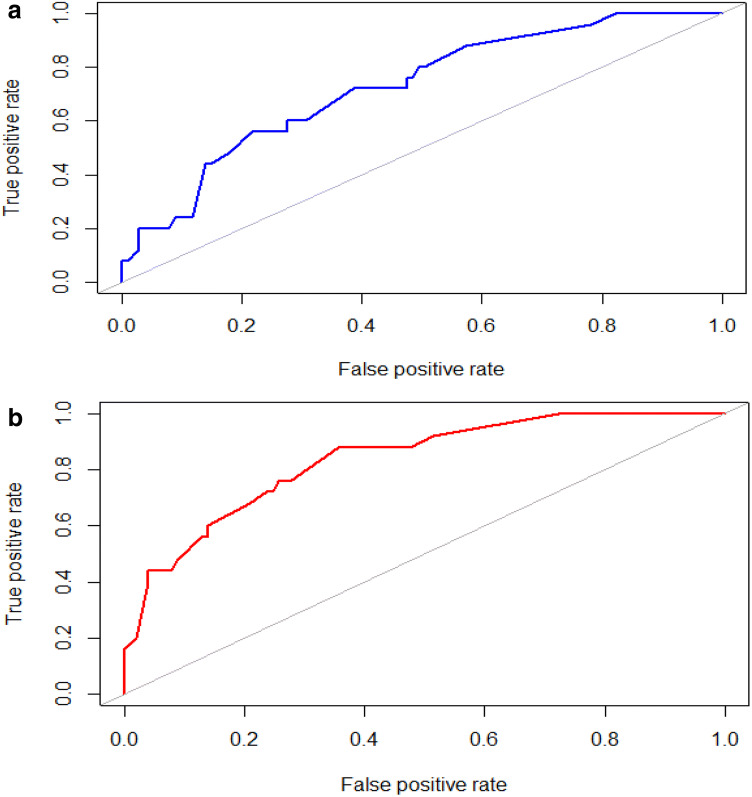
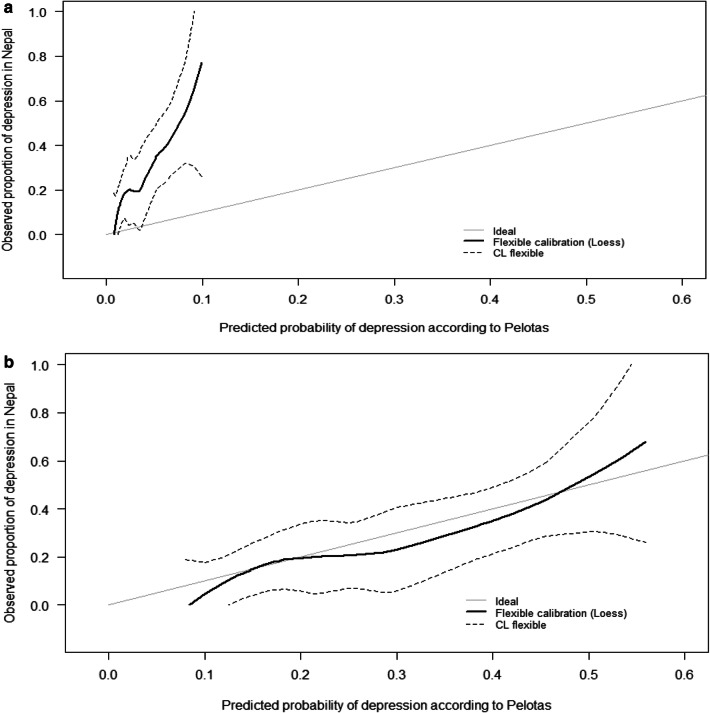
The burden of adolescent depression is high in low- and middle-income countries (LMICs), yet research into prevention is lacking. Development and validation of models to predict individualized risk of depression among adolescents in LMICs is rare but crucial to ensure appropriate targeting of preventive interventions. We assessed the ability of a model developed in Brazil, a middle-income country, to predict depression in an existing culturally different adolescent cohort from Nepal, a low-income country with a large youth population with high rates of depression. Data were utilized from the longitudinal study of 258 former child soldiers matched with 258 war-affected civilian adolescents in Nepal. Prediction modelling techniques were employed to predict individualized risk of depression at age 18 or older in the Nepali cohort using a penalized logistic regression model. Following a priori exclusions for prior depression and age, 55 child soldiers and 71 war-affected civilians were included in the final analysis. The model was well calibrated, had good overall performance, and achieved good discrimination between depressed and non-depressed individuals with an area under the curve (AUC) of 0.73 (bootstrap-corrected 95% confidence interval 0.62-0.83). The Brazilian model comprising seven matching sociodemographic predictors, was able to stratify individualized risk of depression in a Nepali adolescent cohort. Further testing of the model's performance in larger socio-culturally diverse samples in other geographical regions should be attempted to test the model's wider generalizability.
Keywords: Adolescence; External validation; LMIC; Mental health; Prediction model; Risk calculator.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- World Health Organization . Depression and other common mental disorders: global health estimates (No. WHO/MSD/MER/2017.2) Geneva: World Health Organization; 2017.
-
- Curry J, Silva S, Rohde P, Ginsburg G, Kratochvil C, Simons A, Kirchner J, May D, Kennard B, Mayes T, Feeny N, Albano A, Lavanier S, Reinecke M, Jacobs R, Becker-Weidman E, Weller E, Emslie G, Walkup J, Kastelic E, Burns B, Wells K, March J. Recovery and recurrence following treatment for adolescent major depression. Arch Gen Psychiatry. 2011;68:263–269. doi: 10.1001/archgenpsychiatry.2010.150. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
