

Efficacy and Safety of Remogliflozin Etabonate, a New Sodium Glucose Co-Transporter-2 Inhibitor, in Patients with Type 2 Diabetes Mellitus: A 24-Week, Randomized, Double-Blind, Active-Controlled Trial
- PMID: 32162274
- PMCID: PMC7165159
- DOI: 10.1007/s40265-020-01285-0
Efficacy and Safety of Remogliflozin Etabonate, a New Sodium Glucose Co-Transporter-2 Inhibitor, in Patients with Type 2 Diabetes Mellitus: A 24-Week, Randomized, Double-Blind, Active-Controlled Trial
Abstract
Background: Metformin is the first-line treatment for type 2 diabetes mellitus (T2DM), but many patients either cannot tolerate it or cannot achieve glycemic control with metformin alone, so treatment with other glucose-lowering agents in combination with metformin is frequently required. Remogliflozin etabonate, a novel agent, is an orally bioavailable prodrug of remogliflozin, which is a potent and selective sodium-glucose co-transporter-2 inhibitor.
Objective: Our objective was to evaluate the efficacy and safety of remogliflozin etabonate compared with dapagliflozin in subjects with T2DM in whom a stable dose of metformin as monotherapy was providing inadequate glycemic control.
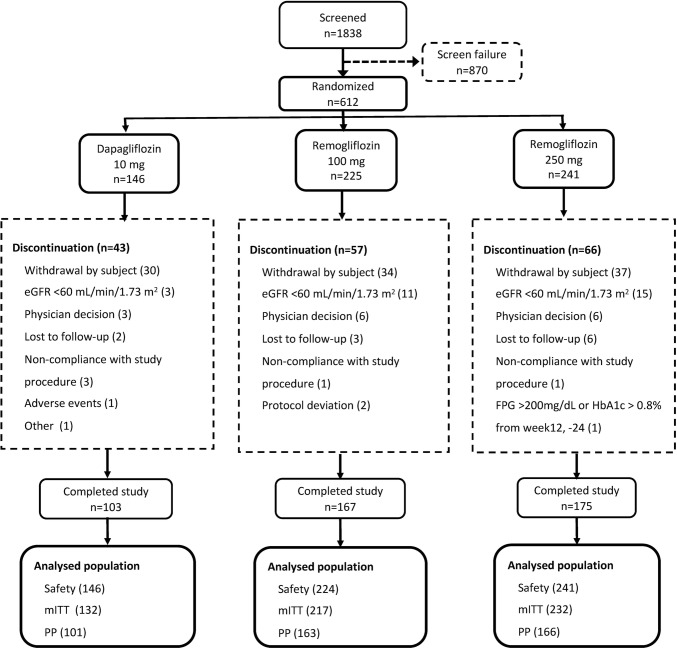
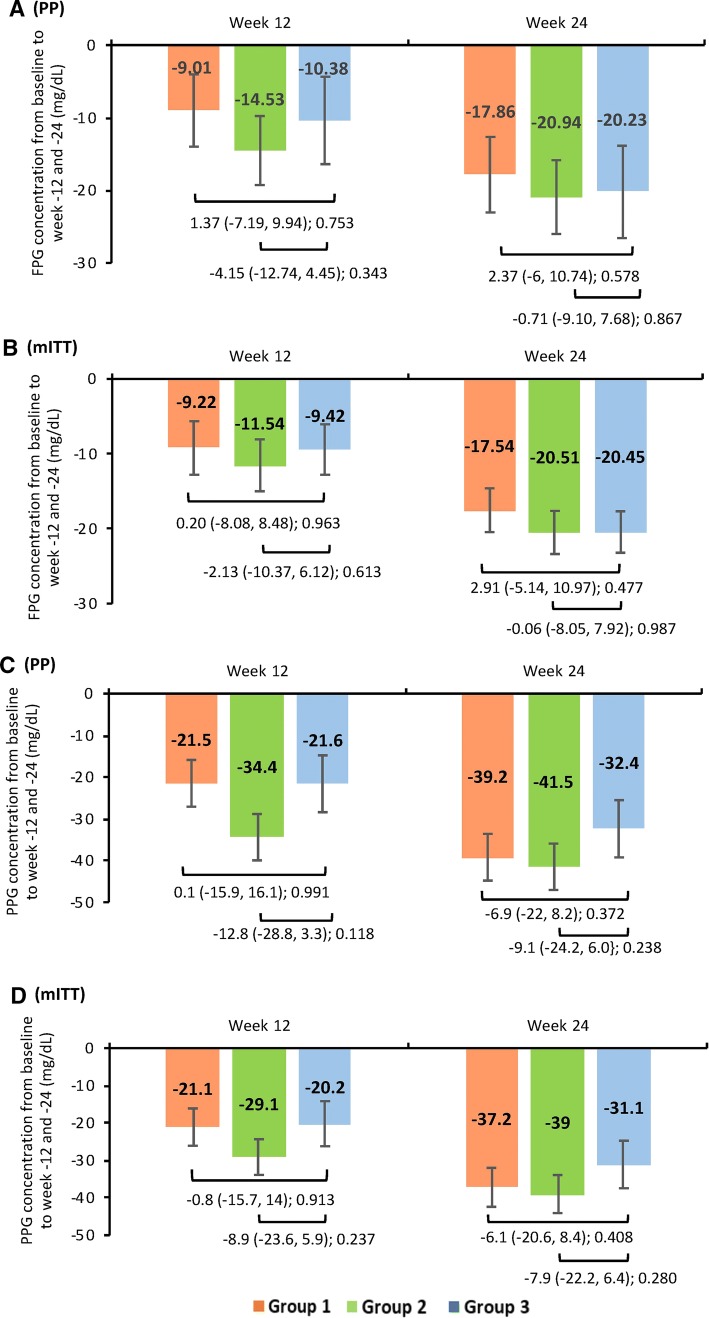
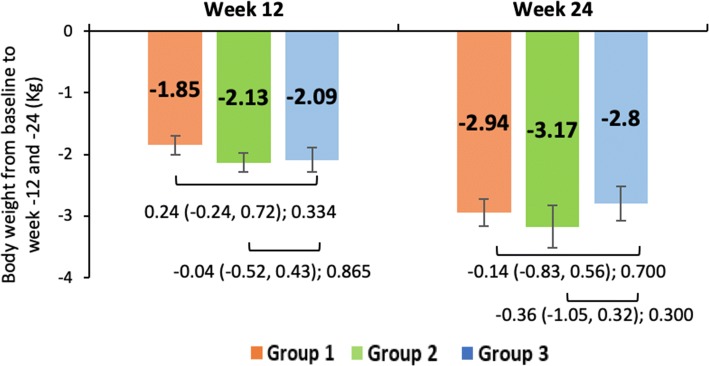
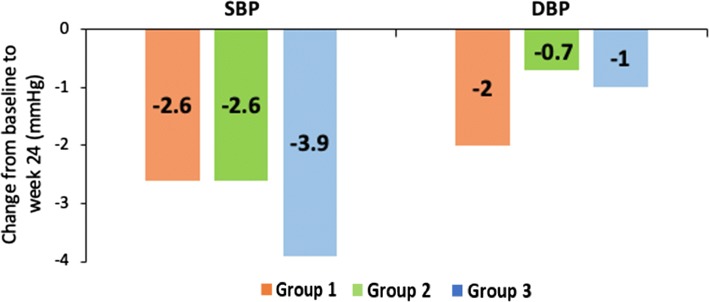
Methods: A 24-week randomized, double-blind, double-dummy, active-controlled, three-arm, parallel-group, multicenter, phase III study was conducted in India. Patients aged ≥ 18 and ≤ 65 years diagnosed with T2DM, receiving metformin ≥ 1500 mg/day, and with glycated hemoglobin (HbA1c) levels ≥ 7 to ≤ 10% at screening were randomized into three groups. Every patient received metformin ≥ 1500 mg and either remogliflozin etabonate 100 mg twice daily (BID) (group 1, n = 225) or remogliflozin etabonate 250 mg BID (group 2, n = 241) or dapagliflozin 10 mg once daily (QD) in the morning and placebo QD in the evening (group 3, n = 146). The patients were followed-up at weeks 1 and 4 and at 4-week intervals thereafter until week 24. The endpoints included mean change in HbA1c (primary endpoint, noninferiority margin = 0.35), fasting plasma glucose (FPG), postprandial plasma glucose (PPG), bodyweight, blood pressure, and fasting lipids. Treatment-emergent adverse events (TEAEs), safety laboratory values, electrocardiogram, and vital signs were evaluated.
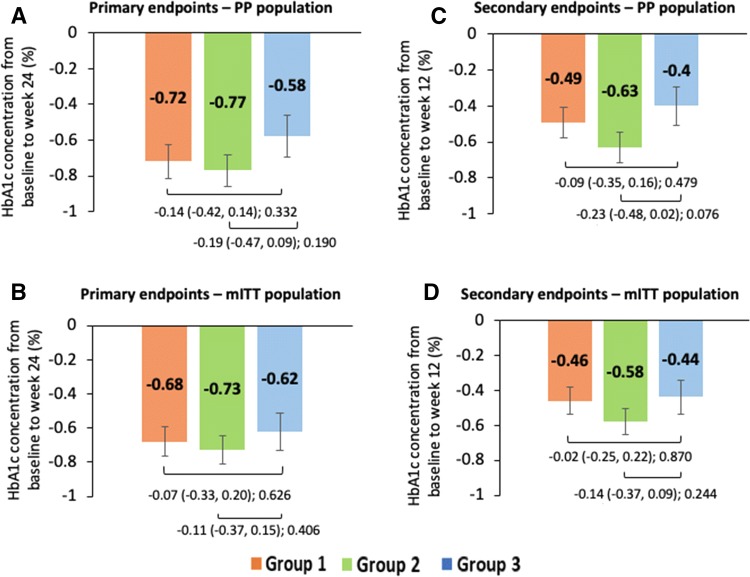
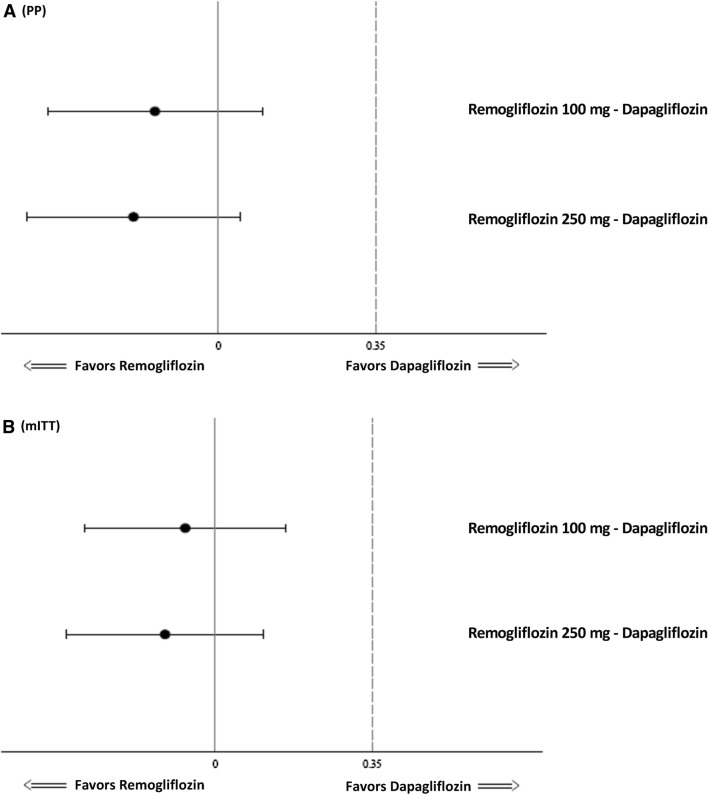
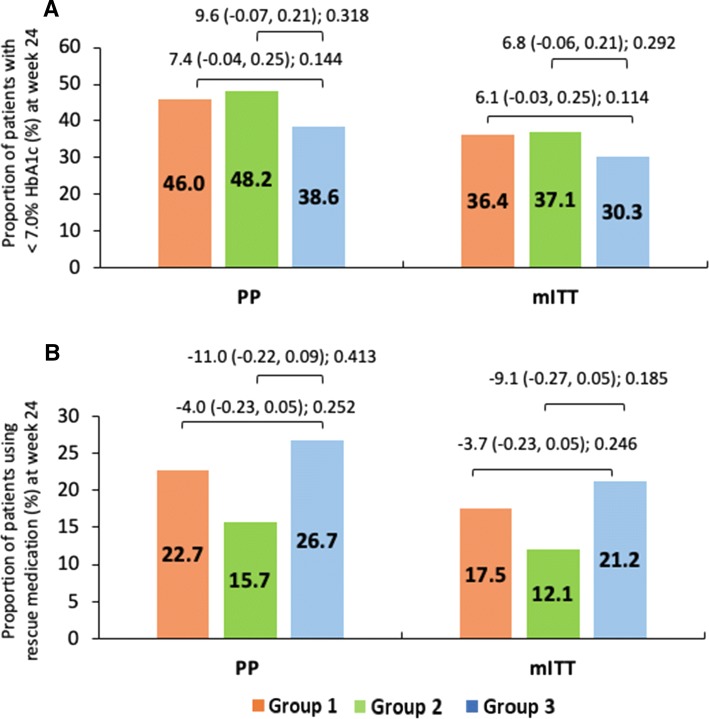
Results: Of 612 randomized patients, 167 (group 1), 175 (group 2), and 103 (group 3) patients with comparable baseline characteristics completed the study. Mean change ± standard error (SE) in HbA1c from baseline to week 24 was - 0.72 ± 0.09, - 0.77 ± 0.09, and - 0.58 ± 0.12% in groups 1, 2, and 3, respectively. The difference in mean HbA1c of group 1 versus group 3 (- 0.14%, 90% confidence interval [CI] - 0.38 to 0.10) and group 2 versus group 3 (- 0.19%; 90% CI - 0.42 to 0.05) was noninferior to that in group 3 (p < 0.001). No significant difference was found between group 1 or group 2 and group 3 in change in FPG, PPG, and bodyweight. The overall incidence of TEAEs was comparable across study groups (group 1 = 32.6%, group 2 = 34.4%, group 3 = 29.5%), including adverse events (AEs) of special interest (hypoglycemic events, urinary tract infection, genital fungal infection). Most TEAEs were mild to moderate in intensity, and no severe AEs were reported.
Conclusion: This study demonstrated the noninferiority of remogliflozin etabonate 100 and 250 mg compared with dapagliflozin, from the first analysis of an initial 612 patients. Remogliflozin etabonate therefore may be considered an effective and well-tolerated alternative treatment option for glycemic control in T2DM.
Trial registration: CTRI/2017/07/009121.
Conflict of interest statement
Rahul Kodgule, Monika Tandon, Sivakumar Vaidyanathan, Amol Pendse, Rajesh Gaikwad, Sagar Katare, Sachin Suryawanshi, and Hanmant Barkate are employees of Glenmark Pharmaceuticals Limited. Mala Dharmalingam, S.R Aravind, Hemant Thacker, S. Paramesh, Brij Mohan, Manoj Chawla, Arthur Asirvatham, Ramesh Goyal, Jayashri Shembalkar, R. Balamurugan, Pradnya Kadam, and Hansraj Alva have no conflicts of interest that are directly relevant to the content of this article.
Figures
References
-
- International Diabetes Federation. IDF Diabetes Atlas, 8th edn. Brussels: International Diabetes Federation. 2017. http://www.diabetesatlas.org. Accessed 27 July 2019.
-
- International Diabetes Federation Global guideline for type 2 diabetes. http://www.idf.org/global-guideline-type-2-diabetes-2012. Accessed 5 Sep 2013.
-
- National Institute for Health and Clinical Excellence Type 2 diabetes: The management of type 2 diabetes (NICE clinical guideline 87). http://www.nice.org.uk/guidance/CG87. Accessed 15 Aug 2013.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
