

Fracture risk assessment and clinical decision making for patients with metastatic bone disease
- PMID: 32162711
- PMCID: PMC7225068
- DOI: 10.1002/jor.24660
Fracture risk assessment and clinical decision making for patients with metastatic bone disease
Abstract
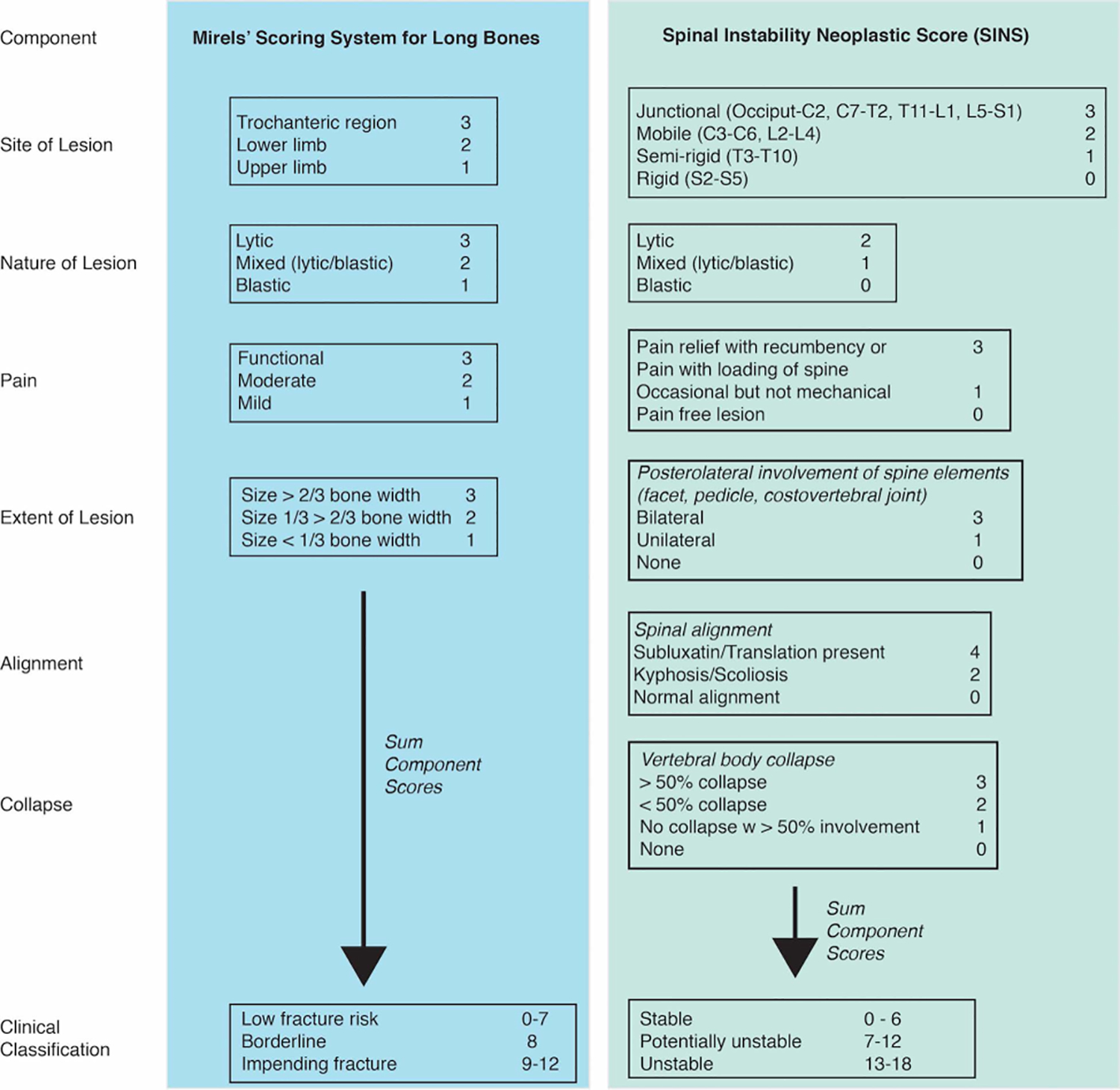
Metastatic breast, prostate, lung, and other cancers often affect bone, causing pain, increasing fracture risk, and decreasing function. Management of metastatic bone disease (MBD) is clinically challenging when there is potential but uncertain risk of pathological fracture. Management of MBD has become a major focus within orthopedic oncology with respect to fracture and impending fracture care. If impending skeletal-related events (SREs), particularly pathologic fracture, could be predicted, increasing evidence suggests that prophylactic surgical treatment improves patient outcomes. However, current fracture risk assessment and radiographic metrics do not have high accuracy and have not been combined with relevant patient survival tools. This review first explores the prevalence, incidence, and morbidity of MBD and associated SREs for different cancer types. Strengths and limitations of current fracture risk scoring systems for spinal stability and long bone fracture are highlighted. More recent computed tomography (CT)-based structural rigidity analysis (CTRA) and finite element (FE) analysis methods offer advantages of increased specificity (true negative rate), but are limited in availability. Other fracture prediction approaches including parametric response mapping and positron emission tomography/computed tomography measures show early promise. Substantial new information to inform clinical decision-making includes measures of survival, clinical benefits, and economic analysis of prophylactic treatment compared to after-fracture stabilization. Areas of future research include use of big data and machine learning to predict SREs, greater access and refinement of CTRA/FE approaches, combination of clinical survival prediction tools with radiographically based fracture risk assessment, and net benefit analysis for fracture risk assessment and prophylactic treatment.
Keywords: clinical decision making; fracture risk; metastatic bone disease; prophylactic stabilization; skeletal-related events.
© 2020 Orthopaedic Research Society. Published by Wiley Periodicals, Inc.
Figures



Similar articles
-
Does CT-based Rigidity Analysis Influence Clinical Decision-making in Simulations of Metastatic Bone Disease?Clin Orthop Relat Res. 2016 Mar;474(3):652-9. doi: 10.1007/s11999-015-4371-1. Clin Orthop Relat Res. 2016. PMID: 26022114 Free PMC article.
-
CT-based Structural Rigidity Analysis Is More Accurate Than Mirels Scoring for Fracture Prediction in Metastatic Femoral Lesions.Clin Orthop Relat Res. 2016 Mar;474(3):643-51. doi: 10.1007/s11999-015-4453-0. Clin Orthop Relat Res. 2016. PMID: 26169800 Free PMC article.
-
Finite element analysis potentially identifies nonessential prophylactic stabilization in femurs with metastatic disease.Proc Inst Mech Eng H. 2022 Sep;236(9):1297-1308. doi: 10.1177/09544119221109740. Epub 2022 Jul 5. Proc Inst Mech Eng H. 2022. PMID: 35787214
-
Fracture Risk of Long Bone Metastases: A Review of Current and New Decision-Making Tools for Prophylactic Surgery.Cancers (Basel). 2021 Jul 21;13(15):3662. doi: 10.3390/cancers13153662. Cancers (Basel). 2021. PMID: 34359563 Free PMC article. Review.
-
Impending fracture associated with bone destruction.Orthopedics. 1992 May;15(5):547-50. doi: 10.3928/0147-7447-19920501-05. Orthopedics. 1992. PMID: 1589348 Review.
Cited by
-
Patient-specific finite element modeling for fracture risk prediction in a canine model of osteosarcoma.Ann Transl Med. 2024 Feb 1;12(1):5. doi: 10.21037/atm-23-1699. Epub 2023 Dec 11. Ann Transl Med. 2024. PMID: 38304903 Free PMC article.
-
Internal validation of modified Mirels' scoring system for pathologic femur fractures.BMC Musculoskelet Disord. 2024 Sep 6;25(1):719. doi: 10.1186/s12891-024-07836-w. BMC Musculoskelet Disord. 2024. PMID: 39243083 Free PMC article.
-
Finite Element Model-Computed Mechanical Behavior of Femurs with Metastatic Disease Varies Between Physiologic and Idealized Loading Simulations.Biomed Eng Comput Biol. 2023 Mar 31;14:11795972231166240. doi: 10.1177/11795972231166240. eCollection 2023. Biomed Eng Comput Biol. 2023. PMID: 37020922 Free PMC article.
-
Prognostic assessment of osteolytic lesions and mechanical properties of bones bearing breast cancer using neural network and finite element analysis☆.Mechanobiol Med. 2025 Mar 30;3(2):100130. doi: 10.1016/j.mbm.2025.100130. eCollection 2025 Jun. Mechanobiol Med. 2025. PMID: 40395772 Free PMC article.
-
Breast Cancer Induced Bone Osteolysis Prediction Using Temporal Variational Autoencoders.BME Front. 2022 Apr 2;2022:9763284. doi: 10.34133/2022/9763284. eCollection 2022. BME Front. 2022. PMID: 37850158 Free PMC article.
References
-
- AAOS. 2019. Metastatic Bone Disease. orthoinfo.aaos.org.
-
- Ellis L, Woods LM, Esteve J, et al. 2014. Cancer incidence, survival and mortality: explaining the concepts. Int J Cancer 135:1774–1782. - PubMed
-
- Rogoz B, Houze de l’Aulnoit A, Duhamel A, et al. 2018. Thirty-Year Trends of Survival and Time-Varying Effects of Prognostic Factors in Patients With Metastatic Breast Cancer-A Single Institution Experience. Clin Breast Cancer 18:246–253. - PubMed
-
- Selvaggi G, Scagliotti GV. 2005. Management of bone metastases in cancer: a review. Crit Rev Oncol Hematol 56:365–378. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
