

Multimodal immune phenotyping of maternal peripheral blood in normal human pregnancy
- PMID: 32163376
- PMCID: PMC7205264
- DOI: 10.1172/jci.insight.134838
Multimodal immune phenotyping of maternal peripheral blood in normal human pregnancy
Abstract
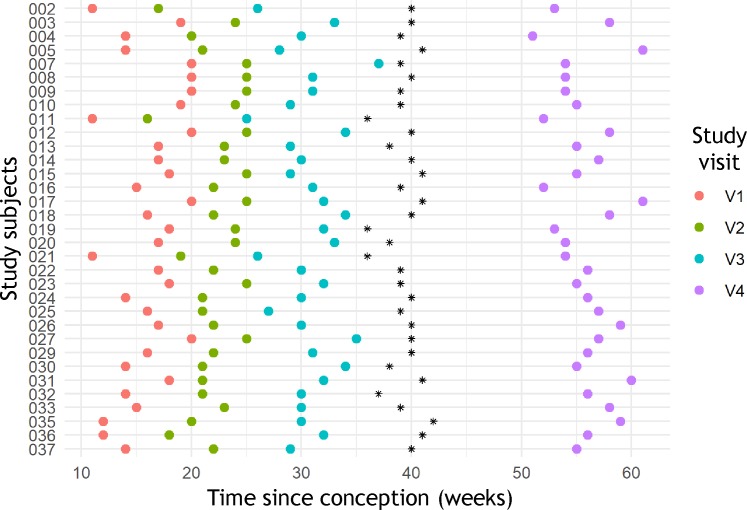
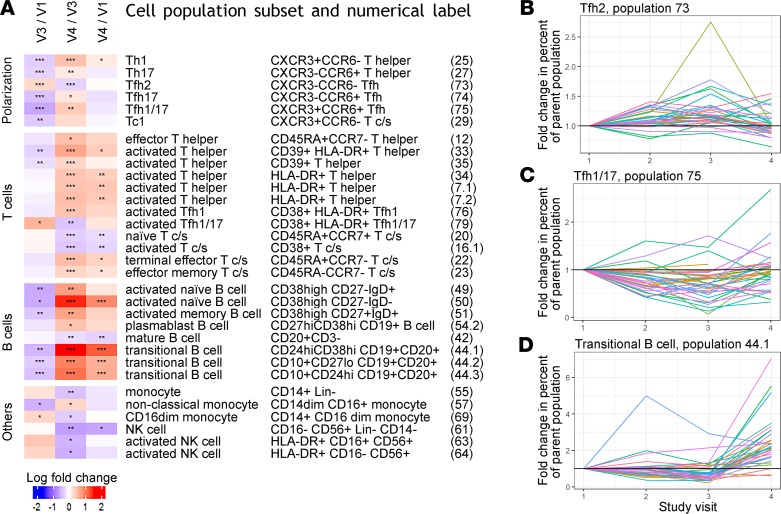
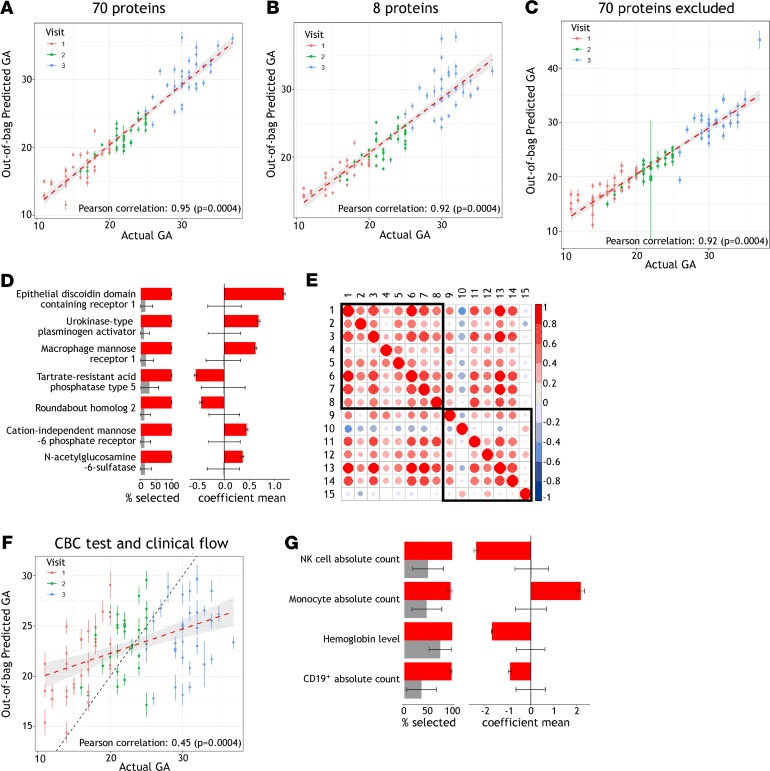
Changes in maternal immunity during pregnancy can result in an altered immune state, and as a natural perturbation, this provides an opportunity to understand functional interactions of the immune system in vivo. We report characterization of maternal peripheral immune phenotypes for 33 longitudinally sampled normal pregnancies, using clinical measurements of complete blood counts and major immune cell populations, as well as high parameter flow cytometry for 30 leukocyte antigens characterizing 79 cell populations, and monitoring of 1305 serum proteins using the SomaLogic platform. Cellular analyses characterized transient changes in T cell polarization and more persistent alterations in T and B cell subset frequencies and activation. Serum proteomic analysis identified a potentially novel set of 7 proteins that are predictive of gestational age: DDR1, PLAU, MRC1, ACP5, ROBO2, IGF2R, and GNS. We further show that gestational age can be predicted from the parameters obtained by complete blood count tests and clinical flow cytometry characterizing 5 major immune cell populations. Inferring gestational age from this routine clinical phenotyping data could be useful in resource-limited settings that lack obstetric ultrasound. Overall, both the cellular and proteomic analyses validate previously reported phenotypic immunological changes of pregnancy and uncover potentially new alterations and predictive markers.
Keywords: Cellular immune response; Immunology; Obstetrics/gynecology; Proteomics; Reproductive Biology.
Conflict of interest statement
Figures
References
-
- Avelino MM, Campos D, Parada JB, Castro AM. Risk factors for Toxoplasma gondii infection in women of childbearing age. Braz J Infect Dis. 2004;8(2):164–174. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
