

Comparing febrile children presenting on and off antibiotics to the emergency department: a retrospective cohort study
- PMID: 32164611
- PMCID: PMC7069000
- DOI: 10.1186/s12887-020-2007-4
Comparing febrile children presenting on and off antibiotics to the emergency department: a retrospective cohort study
Abstract
Background: It is not yet known how antibiotics may affect Serious Bacterial Infections (SBI). Our aim is to describe the presentation, management, and serious bacterial infections (SBI) of febrile children on or off antibiotics.
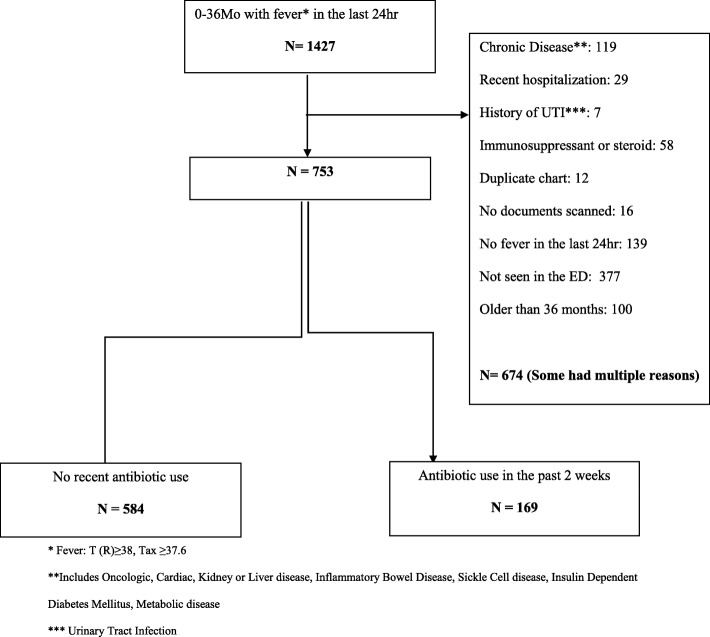
Methods: Retrospective, cohort study of febrile Emergency Department patients, 0-36 months of age, at a single institution, between 2009and 2012.
Results: Seven hundred fifty-three patients were included: 584 in the No-Antibiotics group and 169 (22%) in the Antibiotics group. Age and abnormal lung sounds were predictors for being on antibiotics (OR 2.00 [95% CI 1.23-3.25] and OR 1.04 [95% CI 1.02-1.06] respectively) while female gender, and lower temperatures were negative predictors (OR 0.68 [95%0.47-0.98] and OR 0.47 [95% CI 0.32-0.67] respectively). Antibiotics were prescribed by a physician 89% of the time; the most common one being Amoxicillin/Clavulanic Acid (39%). The antibiotic group got more blood tests (57% vs 45%) and Chest X-Rays (37% vs 25%). Overall, the percent of SBIs (and pneumonias) was statistically the same in both groups (6.5% in the No-antibiotic group VS 3.6%).
Conclusions: Children presenting on antibiotics and off antibiotics were significantly different in their presentation and management, although the overall percentages of SBI were similar in each group. Further investigations into this subgroup of febrile children are needed.
Keywords: Antibiotic use; Febrile children; Serious bacterial infections.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Rui P, Kang K. National hospital ambulatory medical care survey: 2014 emergency department summary tables. 2014.
-
- Craig JC, Williams GJ, Jones M, Codarini M, Macaskill P, Hayen A, et al. The accuracy of clinical symptoms and signs for the diagnosis of serious bacterial infection in young febrile children: prospective cohort study of 15 781 febrile illnesses. BMJ. 2010;340:c1594. doi: 10.1136/bmj.c1594. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
