

Role of ICU-acquired weakness on extubation outcome among patients at high risk of reintubation
- PMID: 32164739
- PMCID: PMC7069045
- DOI: 10.1186/s13054-020-2807-9
Role of ICU-acquired weakness on extubation outcome among patients at high risk of reintubation
Abstract
Background: Whereas ICU-acquired weakness may delay extubation in mechanically ventilated patients, its influence on extubation failure is poorly known. This study aimed at assessing the role of ICU-acquired weakness on extubation failure and the relation between limb weakness and cough strength.
Methods: A secondary analysis of two previous prospective studies including patients at high risk of reintubation after a planned extubation, i.e., age greater than 65 years, with underlying cardiac or respiratory disease, or intubated for more than 7 days prior to extubation. Patients intubated less than 24 h and those with a do-not-reintubate order were not included. Limb and cough strength were assessed by a physiotherapist just before extubation. ICU-acquired weakness was clinically diagnosed as limb weakness defined as Medical Research Council (MRC) score < 48 points and severe weakness as MRC sum-score < 36. Cough strength was assessed using a semi-quantitative 5-Likert scale. Extubation failure was defined as reintubation or death within the first 7 days following extubation.
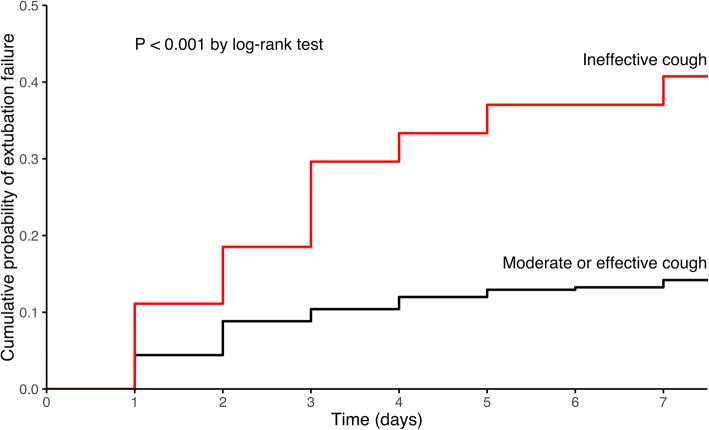
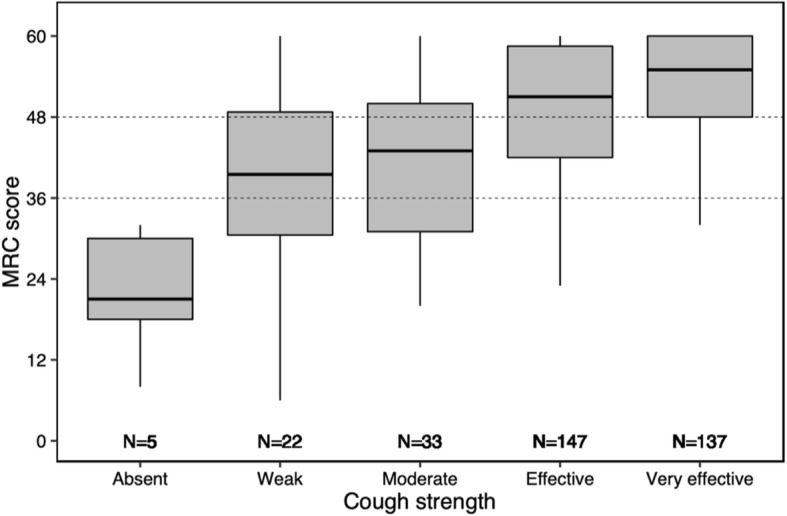
Results: Among 344 patients at high risk of reintubation, 16% experienced extubation failure (56/344). They had greater severity and lower MRC sum-score (41 ± 16 vs. 49 ± 13, p < 0.001) and were more likely to have ineffective cough than the others. The prevalence of ICU-acquired weakness at the time of extubation was 38% (130/244). The extubation failure rate was 12% (25/214) in patients with no limb weakness vs. 18% (12/65) and 29% (19/65) in those with moderate and severe limb weakness, respectively (p < 0.01). MRC sum-score and cough strength were weakly but significantly correlated (rho = 0.28, p < .001). After multivariate logistic regression analyses, the lower the MRC sum-score the greater the risk of reintubation; severe limb weakness was independently associated with extubation failure, even after adjustment on cough strength and severity at admission.
Conclusion: ICU-acquired weakness was diagnosed in 38% in this population of patients at high risk at the time of extubation and was independently associated with extubation failure in the ICU.
Keywords: Extubation; ICU-acquired weakness; Intensive care unit; Mechanical ventilation; Weaning.
Conflict of interest statement
AWT reported receiving grants from the French Ministry of Health, personal fees (payment for lectures, and travel/accommodation expense coverage to attend scientific meetings), and non-financial support from Fisher&Paykel, GE Healthcare, Maquet–Getinge, and Covidien outside the submitted work. The other authors declare that they have no conflict of interest.
Figures

References
-
- Rochwerg Bram, Brochard Laurent, Elliott Mark W., Hess Dean, Hill Nicholas S., Nava Stefano, Navalesi Paolo, Antonelli Massimo, Brozek Jan, Conti Giorgio, Ferrer Miquel, Guntupalli Kalpalatha, Jaber Samir, Keenan Sean, Mancebo Jordi, Mehta Sangeeta, Raoof Suhail. Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. European Respiratory Journal. 2017;50(2):1602426. doi: 10.1183/13993003.02426-2016. - DOI - PubMed
-
- Thille AW, Muller G, Gacouin A, Coudroy R, Demoule A, Sonneville R, Beloncle F, Girault C, Dangers L, Lautrette A, et al. High-flow nasal cannula oxygen therapy alone or with non-invasive ventilation during the weaning period after extubation in ICU: the prospective randomised controlled HIGH-WEAN protocol. BMJ Open. 2018;8(9):e023772. - PMC - PubMed
-
- Thille AW, Muller G, Gacouin A, Coudroy R, Decavele M, Sonneville R, Beloncle F, Girault C, Dangers L, Lautrette A, et al. Effect of postextubation high-flow nasal oxygen with noninvasive ventilation vs high-flow nasal oxygen alone on Reintubation among patients at high risk of extubation failure: a randomized clinical trial. Jama. 2019;322(15):1465–1475. doi: 10.1001/jama.2019.14901. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
