

Stem Cell-Derived Cardiomyocytes and Beta-Adrenergic Receptor Blockade in Duchenne Muscular Dystrophy Cardiomyopathy
- PMID: 32164890
- PMCID: PMC9235061
- DOI: 10.1016/j.jacc.2019.12.066
Stem Cell-Derived Cardiomyocytes and Beta-Adrenergic Receptor Blockade in Duchenne Muscular Dystrophy Cardiomyopathy
Abstract
Background: Although cardiomyopathy has emerged as a leading cause of death in Duchenne muscular dystrophy (DMD), limited studies and therapies have emerged for dystrophic heart failure.
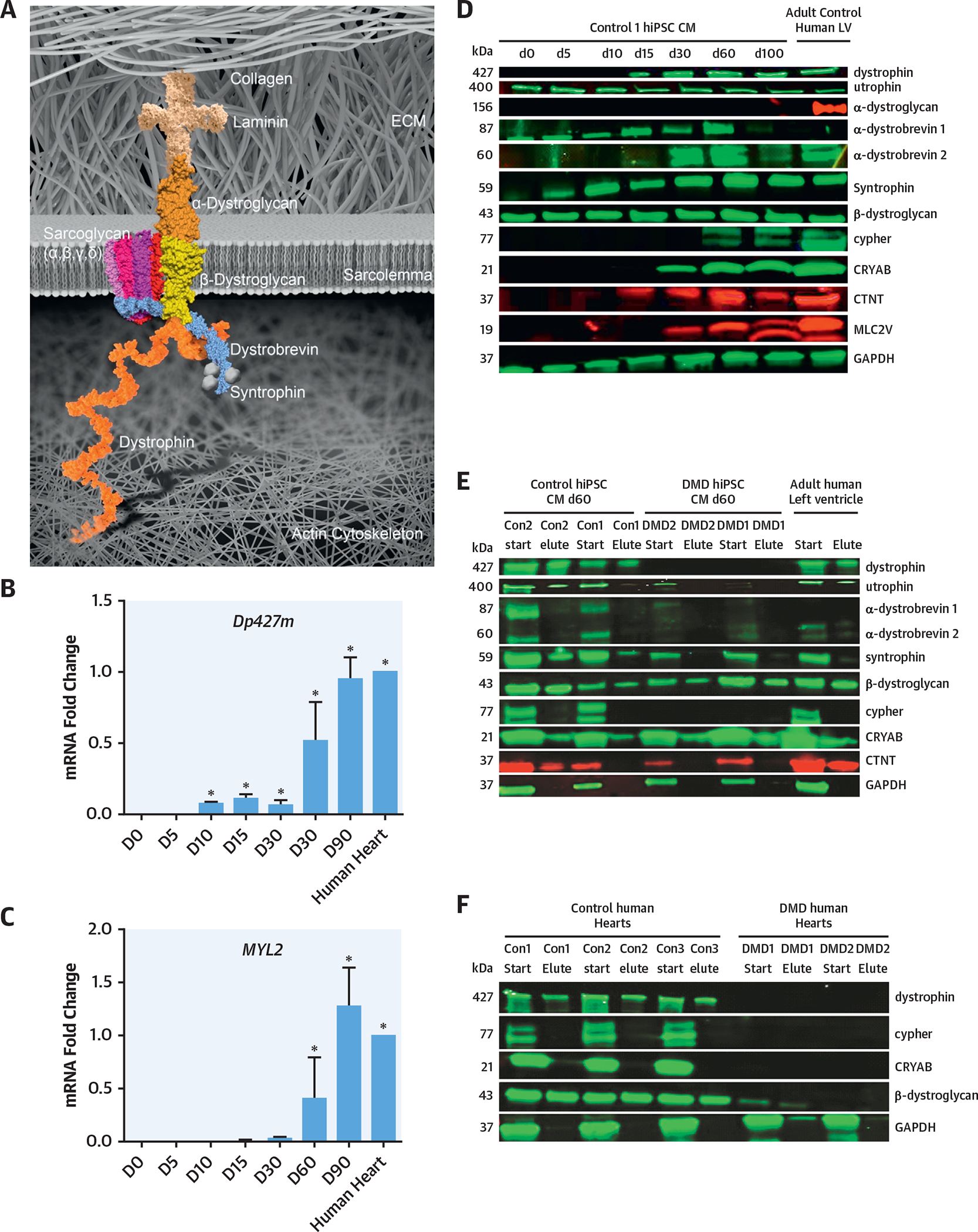
Objectives: The purpose of this study was to model DMD cardiomyopathy using DMD patient-specific human induced pluripotent stem cell (hiPSC)-derived cardiomyocytes and to identify physiological changes and future drug therapies.
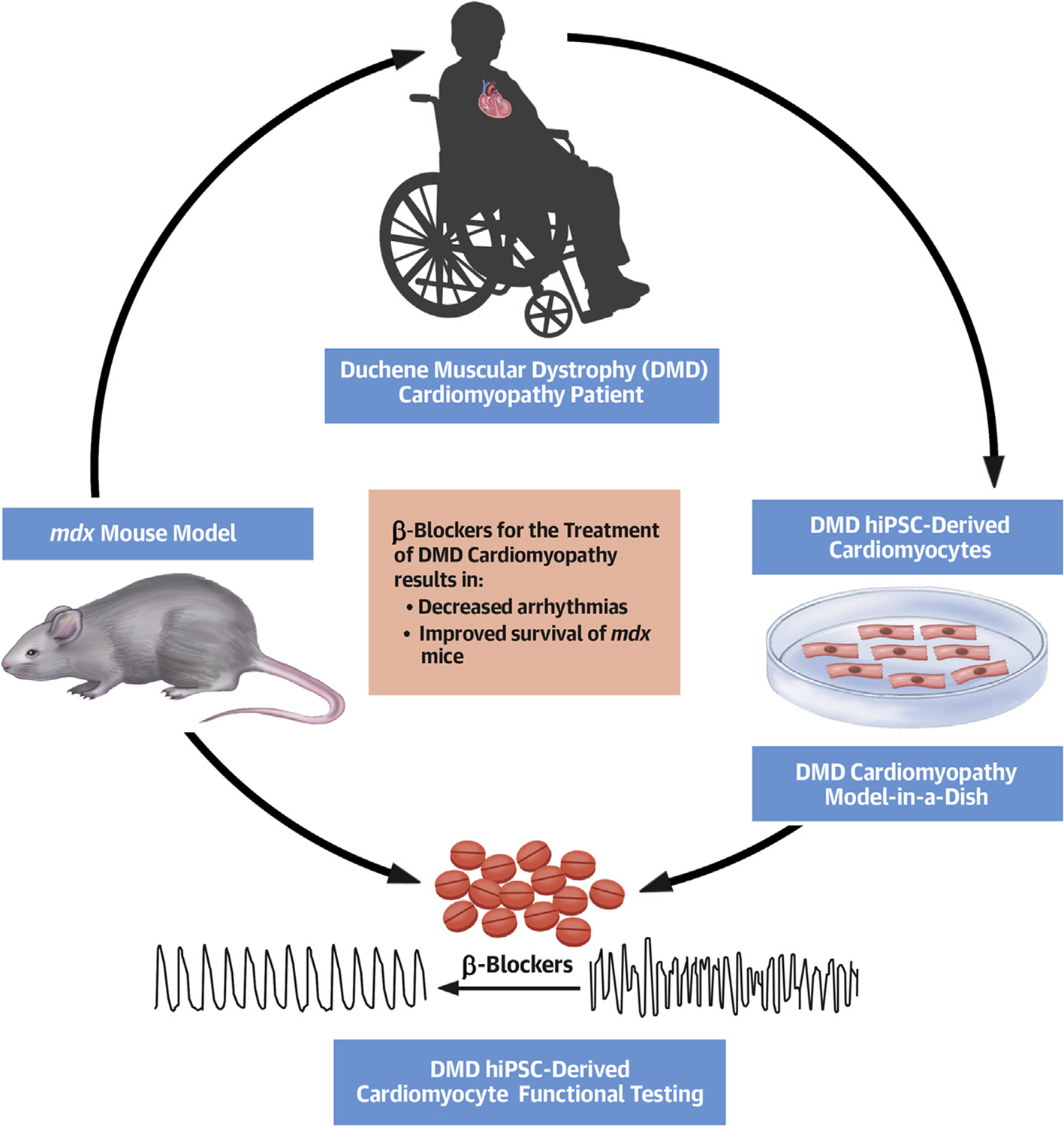
Methods: To explore and define therapies for DMD cardiomyopathy, the authors used DMD patient-specific hiPSC-derived cardiomyocytes to examine the physiological response to adrenergic agonists and β-blocker treatment. The authors further examined these agents in vivo using wild-type and mdx mouse models.
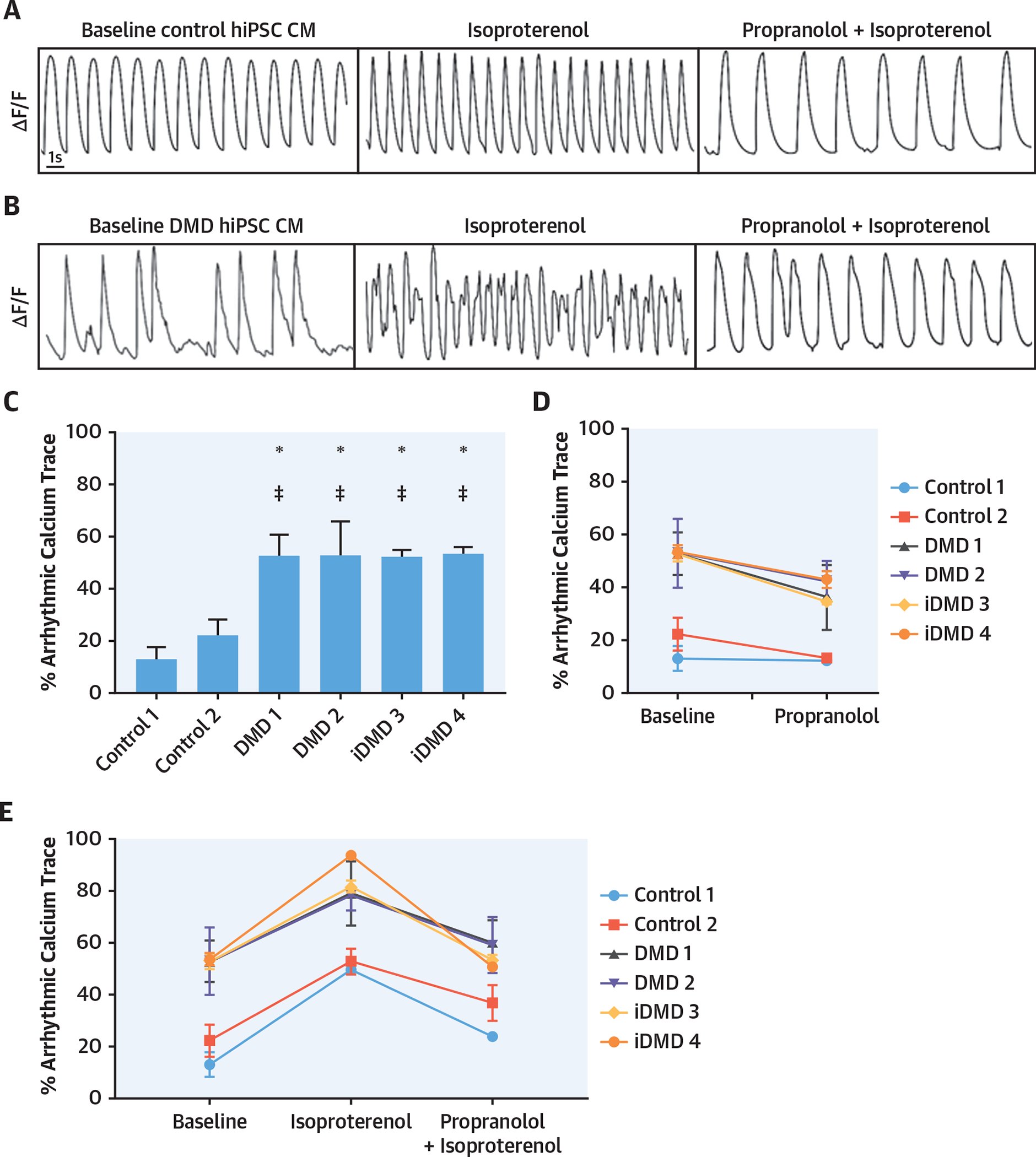
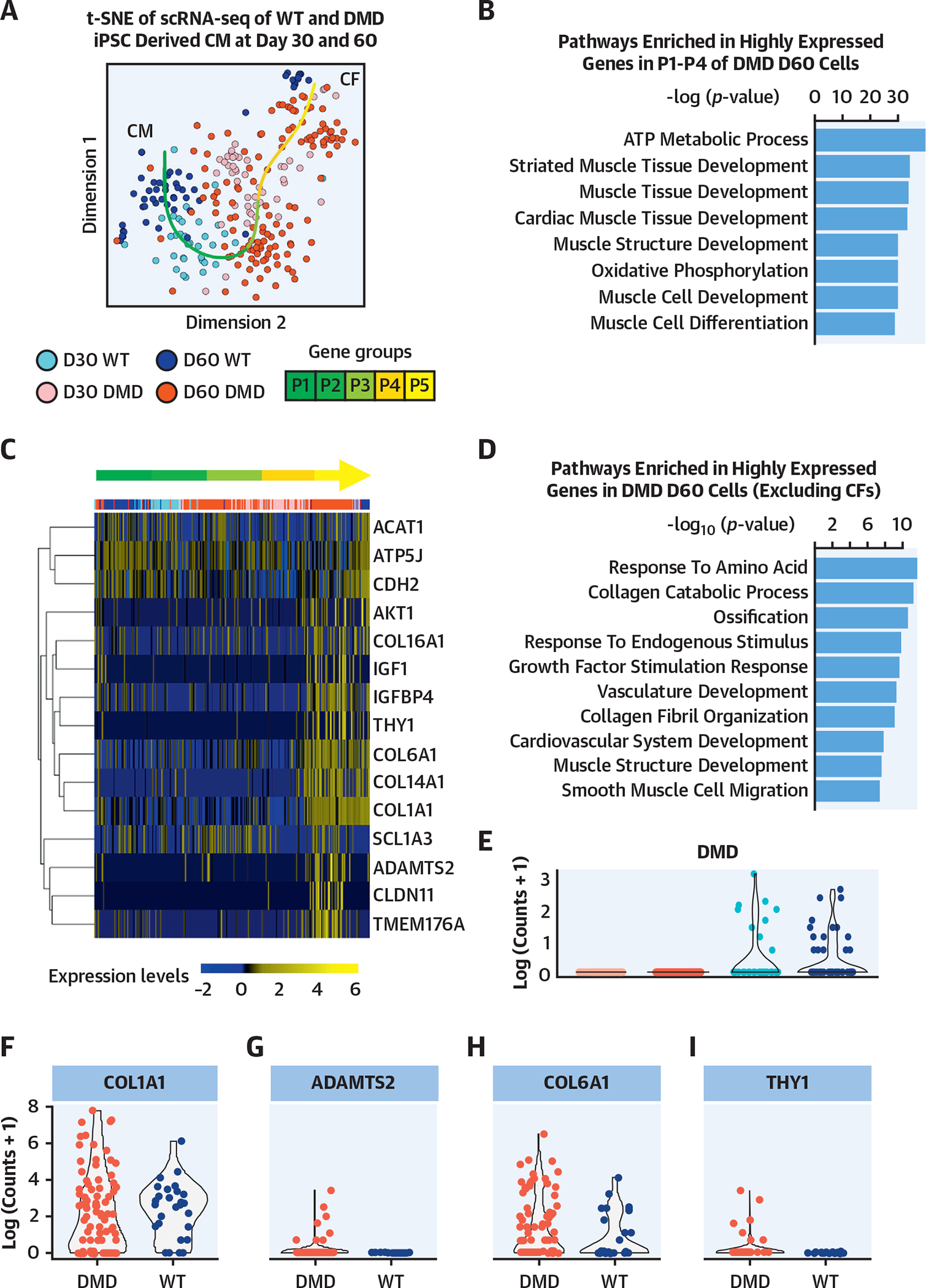
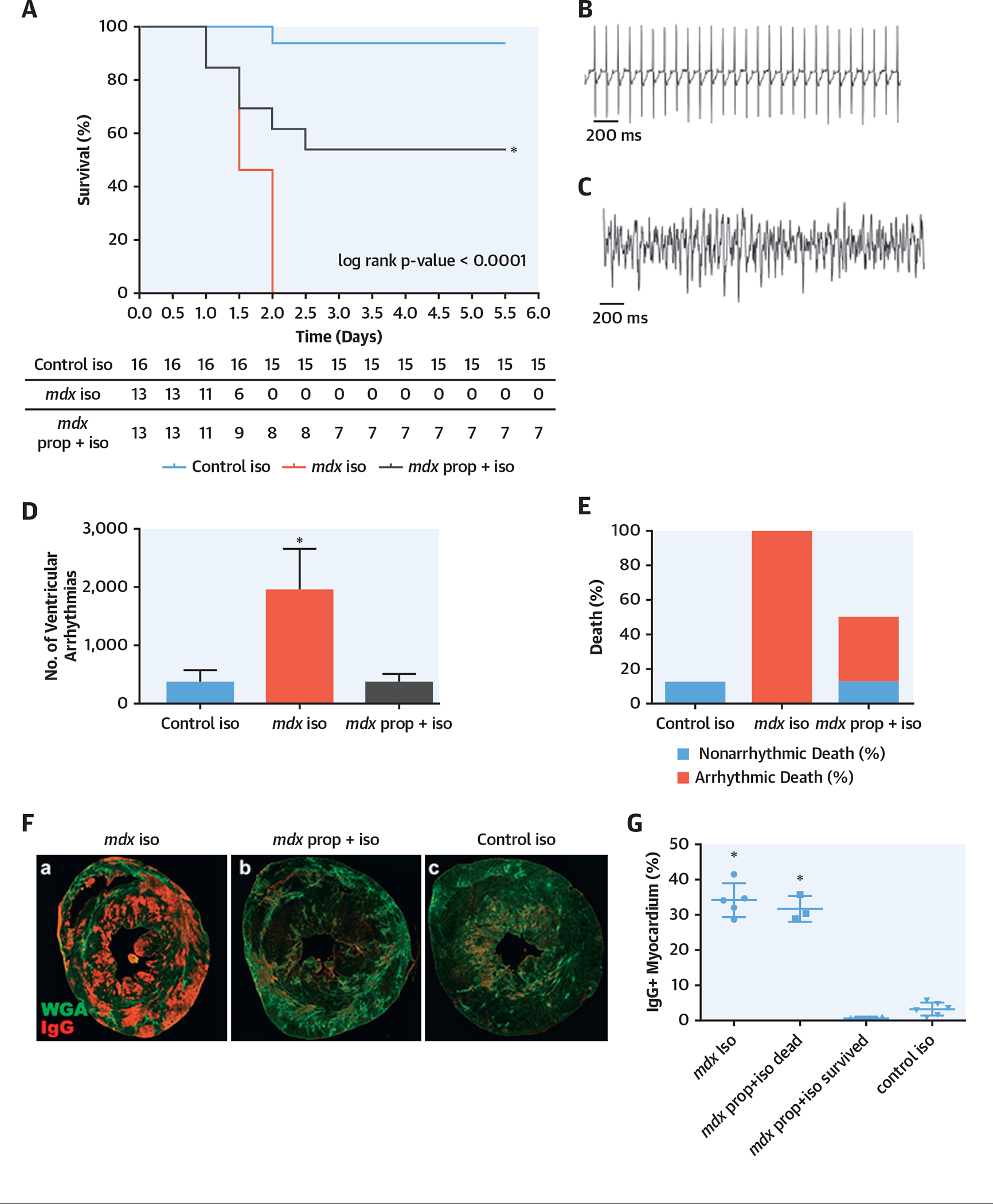
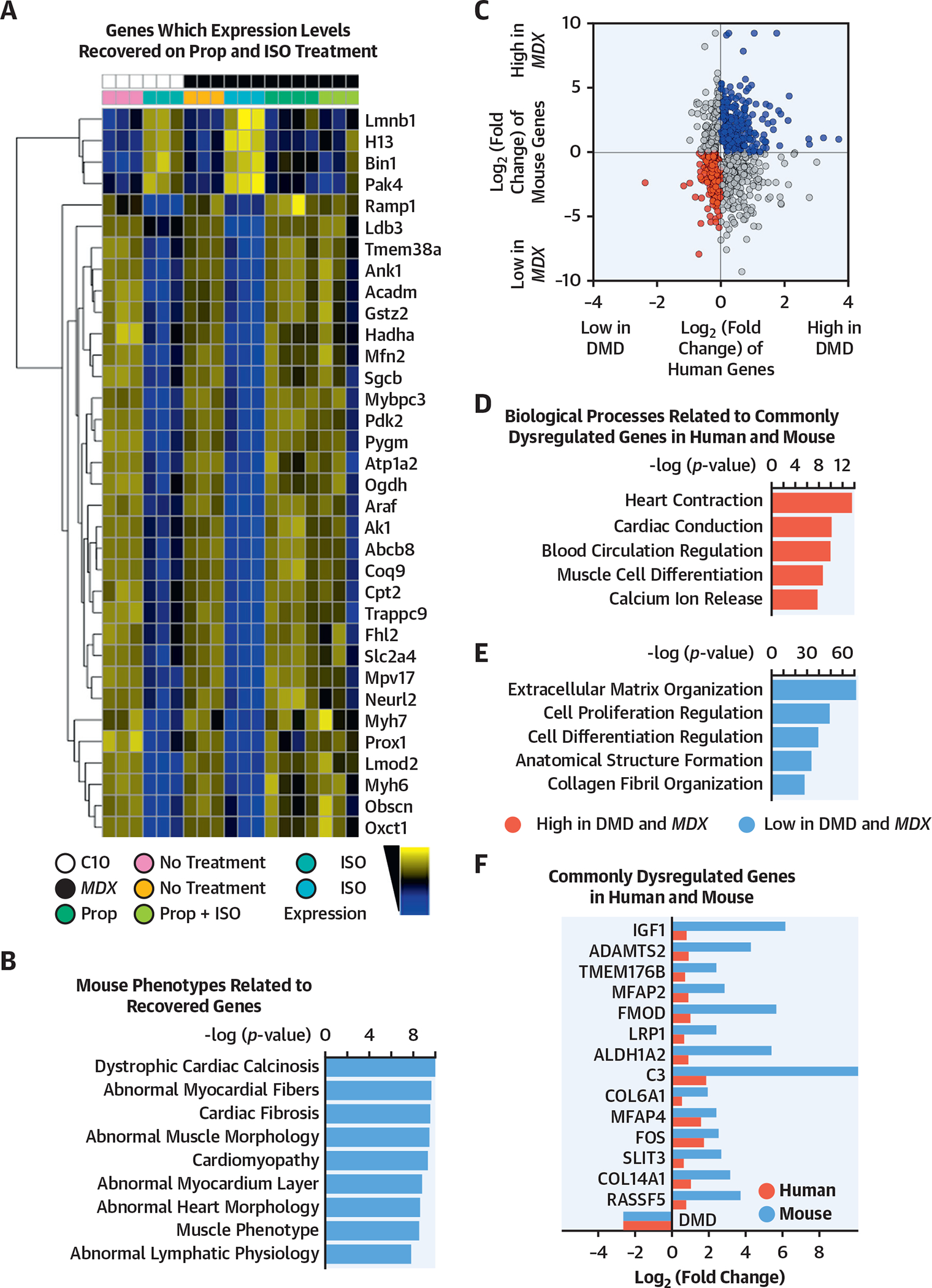
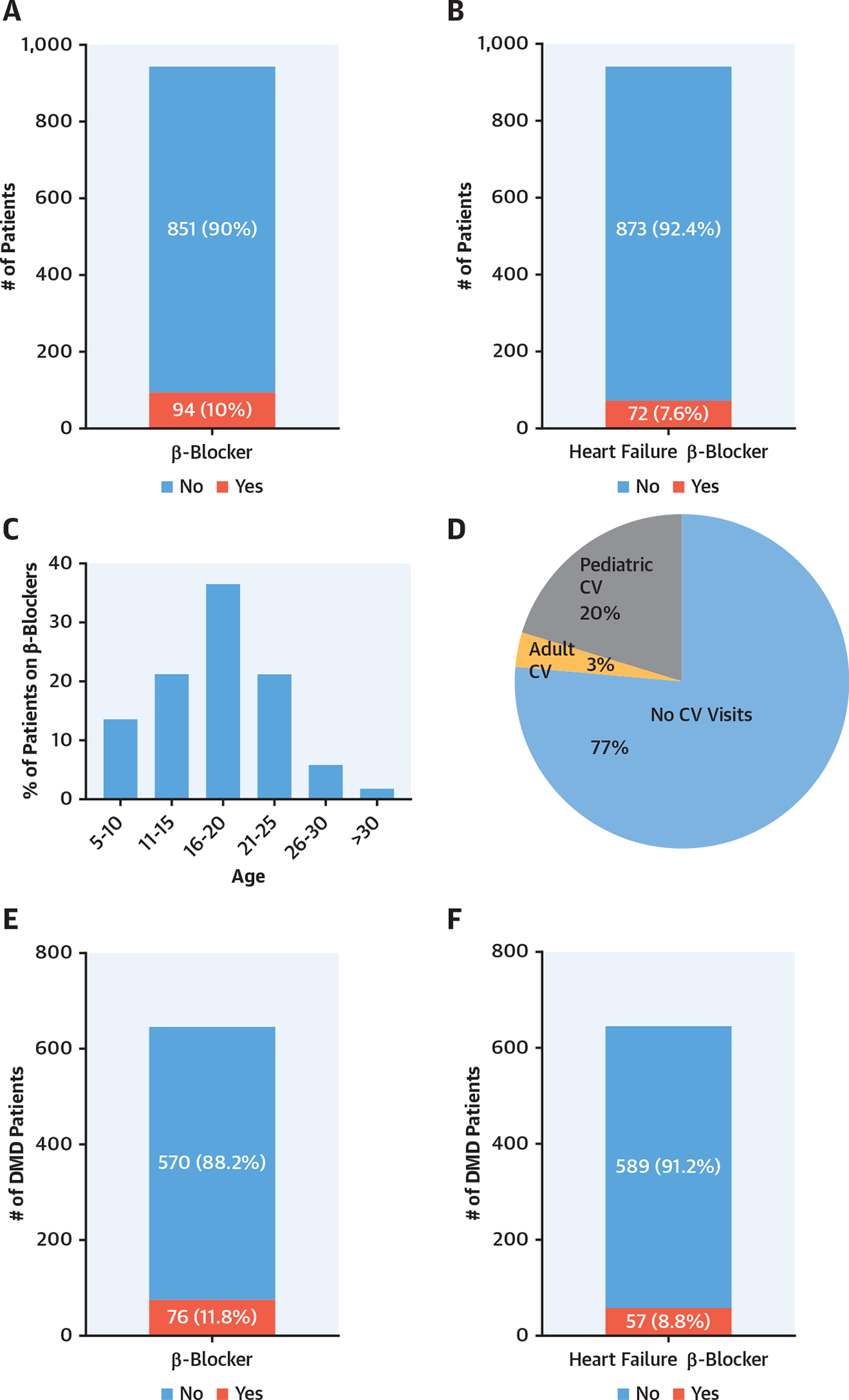
Results: At baseline and following adrenergic stimulation, DMD hiPSC-derived cardiomyocytes had a significant increase in arrhythmic calcium traces compared to isogenic controls. Furthermore, these arrhythmias were significantly decreased with propranolol treatment. Using telemetry monitoring, the authors observed that mdx mice, which lack dystrophin, had an arrhythmic death when stimulated with isoproterenol; the lethal arrhythmias were rescued, in part, by propranolol pre-treatment. Using single-cell and bulk RNA sequencing (RNA-seq), the authors compared DMD and control hiPSC-derived cardiomyocytes, mdx mice, and control mice (in the presence or absence of propranolol and isoproterenol) and defined pathways that were perturbed under baseline conditions and pathways that were normalized after propranolol treatment in the mdx model. The authors also undertook transcriptome analysis of human DMD left ventricle samples and found that DMD hiPSC-derived cardiomyocytes have dysregulated pathways similar to the human DMD heart. The authors further determined that relatively few patients with DMD see a cardiovascular specialist or receive β-blocker therapy.
Conclusions: The results highlight mechanisms and therapeutic interventions from human to animal and back to human in the dystrophic heart. These results may serve as a prelude for an adequately powered clinical study that examines the impact of β-blocker therapy in patients with dystrophinopathies.
Keywords: Duchenne disease modeling; heart failure; human inducible pluripotent stem cells; muscular dystrophy cardiomyopathy; β-blockers.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Can Patient Pluripotent Stem Cell-Derived Cardiomyocytes Provide Useful Modeling on Arrhythmias of DMD Cardiomyopathy?J Am Coll Cardiol. 2020 Mar 17;75(10):1175-1177. doi: 10.1016/j.jacc.2020.01.038. J Am Coll Cardiol. 2020. PMID: 32164891 No abstract available.
References
-
- Mendell JR, Lloyd-Puryear M. Report of MDA muscle disease symposium on newborn screening for Duchenne muscular dystrophy. Muscle Nerve 2013;48:21–6. - PubMed
-
- Emery AE. The muscular dystrophies. Lancet 2002;359:687–95. - PubMed
-
- Cox GF, Kunkel LM. Dystrophies and heart disease. Curr Opin Cardiol 1997;12:329–43. - PubMed
-
- Kamdar F, Garry DJ. Dystrophin-deficient cardiomyopathy. J Am Coll Cardiol 2016;67:2533–46. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
