

CT Angiography in Evaluating Large-Vessel Occlusion in Acute Anterior Circulation Ischemic Stroke: Factors Associated with Diagnostic Error in Clinical Practice
- PMID: 32165362
- PMCID: PMC7144646
- DOI: 10.3174/ajnr.A6469
CT Angiography in Evaluating Large-Vessel Occlusion in Acute Anterior Circulation Ischemic Stroke: Factors Associated with Diagnostic Error in Clinical Practice
Abstract
Background and purpose: It is currently not completely clear how well radiologists perform in evaluating large-vessel occlusion on CTA in acute ischemic stroke. The purpose of this study was to investigate potential factors associated with diagnostic error.
Materials and methods: Five hundred twenty consecutive patients with a clinical diagnosis of acute ischemic stroke (49.4% men; mean age, 72 years) who underwent CTA to evaluate large-vessel occlusion of the proximal anterior circulation were included. CTA scans were retrospectively reviewed by a consensus panel of 2 neuroradiologists. Logistic regression analysis was performed to investigate the association between several variables and missed large-vessel occlusion at the initial CTA interpretation.
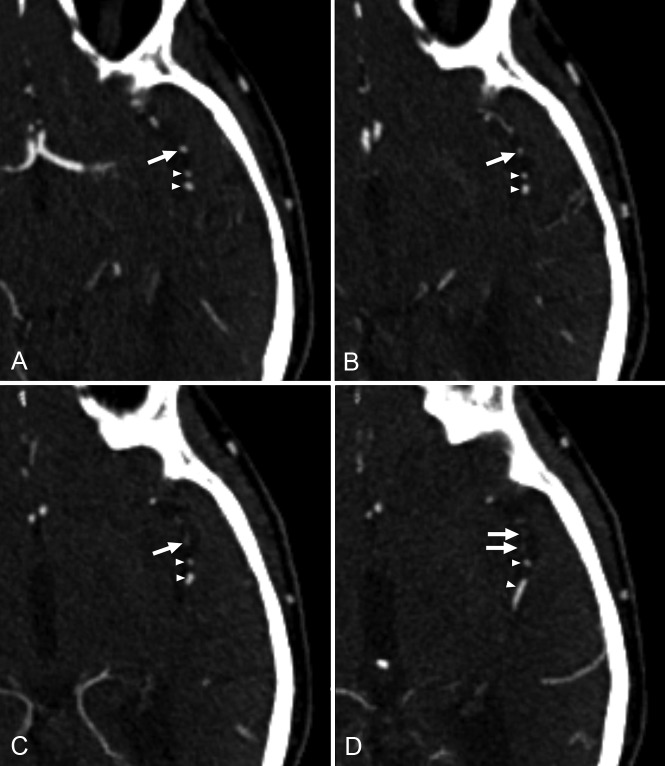
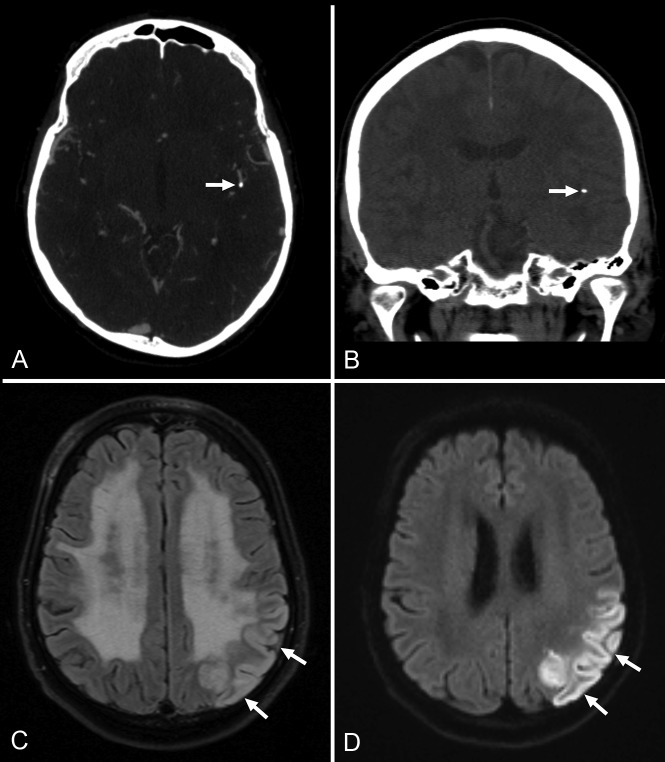
Results: The prevalence of large-vessel occlusion was 16% (84/520 patients); 20% (17/84) of large-vessel occlusions were missed at the initial CTA evaluation. In multivariate analysis, non-neuroradiologists were more likely to miss large-vessel occlusion compared with neuroradiologists (OR = 5.62; 95% CI, 1.06-29.85; P = .04), and occlusions of the M2 segment were more likely to be missed compared with occlusions of the distal internal carotid artery and/or M1 segment (OR = 5.69; 95% CI, 1.44-22.57; P = .01). There were no calcified emboli in initially correctly identified large-vessel occlusions. However, calcified emboli were present in 4 of 17 (24%) initially missed or misinterpreted large-vessel occlusions.
Conclusions: Several factors may have an association with missing a large-vessel occlusion on CTA, including the CTA interpreter (non-neuroradiologists versus neuroradiologists), large-vessel occlusion location (M2 segment versus the distal internal carotid artery and/or M1 segment), and large-vessel occlusion caused by calcified emboli. Awareness of these factors may improve the accuracy in interpreting CTA and eventually improve stroke outcome.
© 2020 by American Journal of Neuroradiology.
Figures
Comment in
-
Missed Medium-Vessel Occlusions on CT Angiography: Make It Easier … Easily!AJNR Am J Neuroradiol. 2020 Sep;41(9):E73-E74. doi: 10.3174/ajnr.A6670. Epub 2020 Jul 9. AJNR Am J Neuroradiol. 2020. PMID: 32646943 Free PMC article. No abstract available.
-
Reply.AJNR Am J Neuroradiol. 2020 Sep;41(9):E75. doi: 10.3174/ajnr.A6700. Epub 2020 Jul 9. AJNR Am J Neuroradiol. 2020. PMID: 32646944 Free PMC article. No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical