

Efficacy and Safety of Flow-Diverter Therapy for Recurrent Aneurysms after Stent-Assisted Coiling
- PMID: 32165365
- PMCID: PMC7144649
- DOI: 10.3174/ajnr.A6476
Efficacy and Safety of Flow-Diverter Therapy for Recurrent Aneurysms after Stent-Assisted Coiling
Abstract
Background and purpose: Flow-diverter treatment for previously stented aneurysms has been reported to be less effective and prone to complications. In this study, we evaluated the effectiveness and safety of flow diverters for recurrent aneurysms after stent-assisted coiling.
Materials and methods: Patients who underwent flow-diverter placement for recurrent aneurysms after stent-assisted coiling between March 2015 and March 2019 were recruited. Clinical and radiographic characteristics and clinical and angiographic outcomes were retrospectively evaluated.
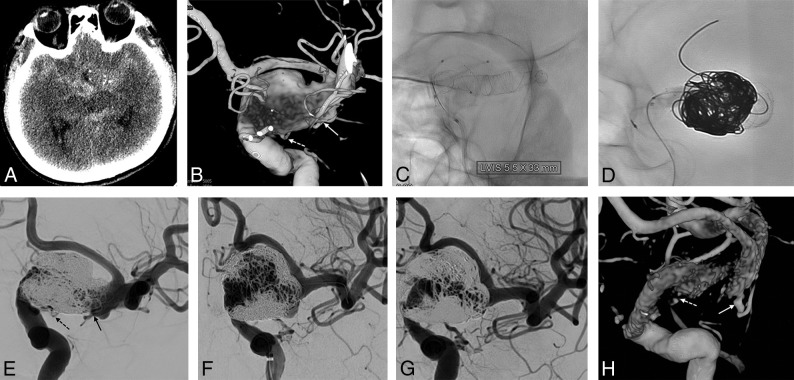
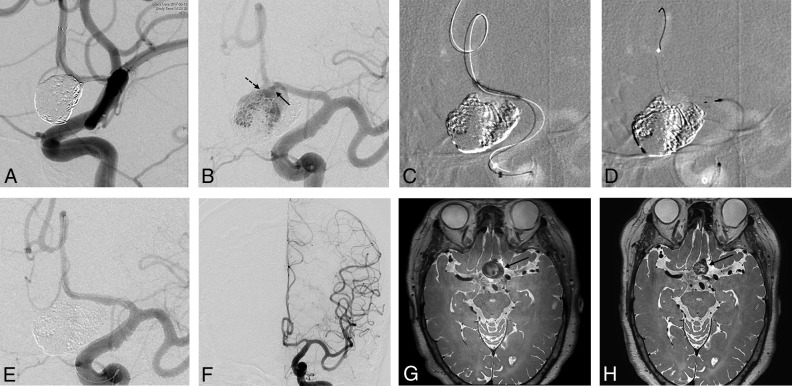
Results: Among 133 patients who underwent flow-diverter insertion, 17 (male/female ratio = 5:12; mean age, 53.8 years) were treated for recurrent aneurysms after stent placement with (n = 16) or without (n = 1) coiling. Eight patients initially presented with subarachnoid hemorrhage; 7, with headache; and 2, with visual field defects. Angiographic morphology included large/giant saccular in 12 patients, dissecting in 2, fusiform in 1, traumatic pseudoaneurysm in 1, and ruptured blood blister-like aneurysm in 1. The duration between the first treatment and flow-diverter placement ranged from 2 weeks to 15 months (median, 6 months). Flow-diverter placement was successful in all cases without any complications. All patients had favorable outcomes (mRS, 0-2), without any newly appearing symptoms. Aneurysms were followed up with conventional angiography at least once in 6-18 months. Sixteen aneurysms showed complete occlusion, and 1 aneurysm was enlarged.
Conclusions: Results from this case series investigating flow-diverter placement for recurrent aneurysms after stent-assisted coiling suggested that the procedure is safe and effective. Further study in a larger population may be warranted.
© 2020 by American Journal of Neuroradiology.
Figures
References
-
- Molyneux AJ, Birks J, Clarke A, et al. . The durability of endovascular coiling versus neurosurgical clipping of ruptured cerebral aneurysms: 18-year follow-up of the UK cohort of the International Subarachnoid Aneurysm Trial (ISAT). Lancet 2015;385:691–97 10.1016/S0140-6736(14)60975-2 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical