

4D-Dynamic Contrast-Enhanced MRI for Preoperative Localization in Patients with Primary Hyperparathyroidism
- PMID: 32165367
- PMCID: PMC7077889
- DOI: 10.3174/ajnr.A6482
4D-Dynamic Contrast-Enhanced MRI for Preoperative Localization in Patients with Primary Hyperparathyroidism
Abstract
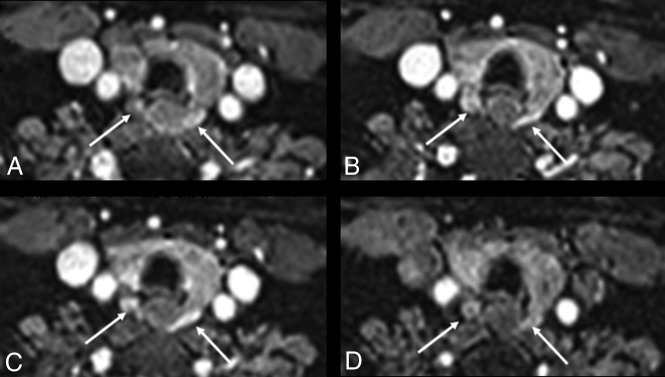
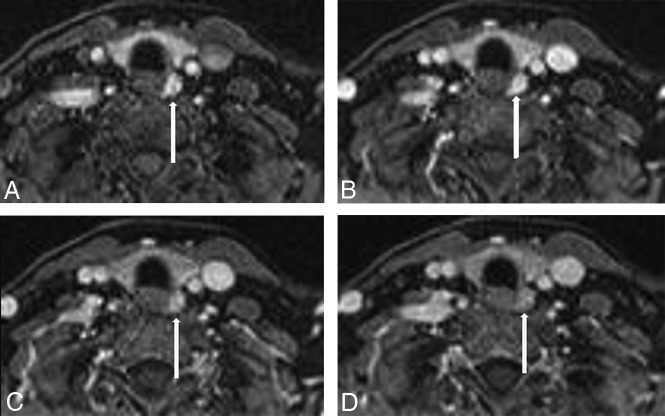
Background and purpose: Our aim was to test the hypothesis that our recently introduced 4D-dynamic contrast-enhanced MR imaging with high spatial and temporal resolution has equivalent accuracy to 4D-CT for preoperative gland localization in primary hyperparathyroidism without requiring exposure to ionizing radiation.
Materials and methods: Inclusion criteria were the following: 1) confirmed biochemical diagnosis of primary hyperparathyroidism, 2) preoperative 4D-dynamic contrast-enhanced MR imaging, and 3) surgical cure with >50% decrease in serum parathyroid hormone intraoperatively. 4D-dynamic contrast-enhanced studies were reviewed independently by 2 neuroradiologists to identify the side, quadrant, and number of abnormal glands, and compared with surgical and pathologic results.
Results: Fifty-four patients met the inclusion criteria: 37 had single-gland disease, and 17, multigland disease (9 with double-gland hyperplasia; 3 with 3-gland hyperplasia; and 5 with 4-gland hyperplasia). Interobserver agreement (κ) for the side (right versus left) was 0.92 for single-gland disease and 0.70 for multigland disease. Interobserver agreement for the quadrant (superior versus inferior) was 0.70 for single-gland disease and 0.69 for multigland disease. For single-gland disease, the gland was correctly located in 34/37 (92%) patients, with correct identification of the side in 37/37 (100%) and the quadrant in 34/37 (92%) patients. For multigland disease, the glands were correctly located in 35/47 (74%) patients, with correct identification of the side in 35/47 (74%) and the quadrant in 36/47 (77%).
Conclusions: The proposed high spatial and temporal resolution 4D-dynamic contrast-enhanced MR imaging provides excellent diagnostic performance for preoperative localization in primary hyperparathyroidism, with correct gland localization of 92% for single-gland disease and 74% in multigland disease, superior to 4D-CT studies.
© 2020 by American Journal of Neuroradiology.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous