

End Points for Clinical Trials in Primary Hyperoxaluria
- PMID: 32165440
- PMCID: PMC7341772
- DOI: 10.2215/CJN.13821119
End Points for Clinical Trials in Primary Hyperoxaluria
Abstract
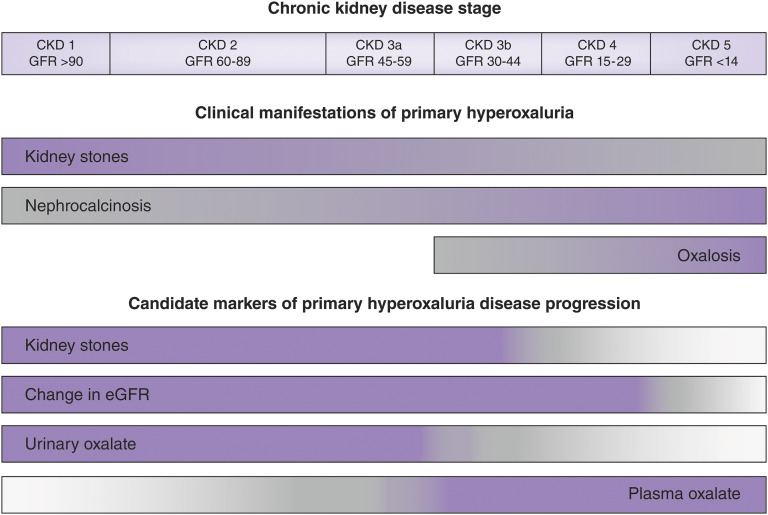
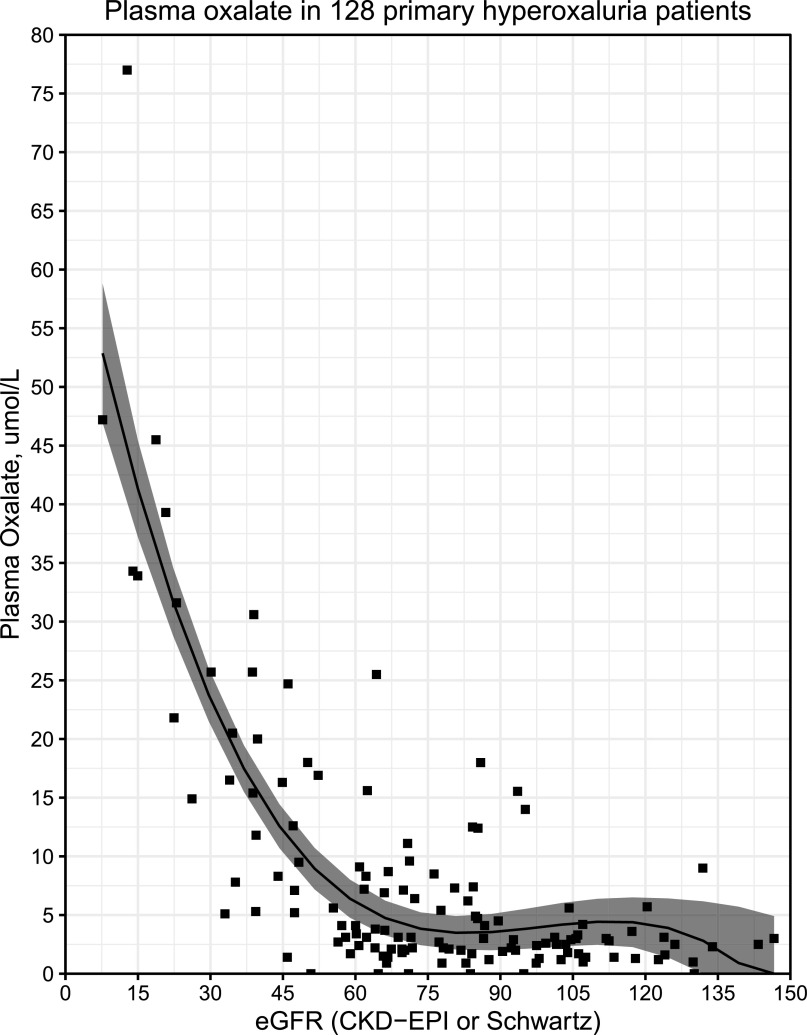
Patients with primary hyperoxaluria experience kidney stones from a young age and can develop progressive oxalate nephropathy. Progression to kidney failure often develops over a number of years, and is associated with systemic oxalosis, intensive dialysis, and often combined kidney and liver transplantation. There are no therapies approved by the Food and Drug Association. Thus, the Kidney Health Initiative, in partnership with the Oxalosis and Hyperoxaluria Foundation, initiated a project to identify end points for clinical trials. A workgroup of physicians, scientists, patients with primary hyperoxaluria, industry, and United States regulators critically examined the published literature for clinical outcomes and potential surrogate end points that could be used to evaluate new treatments. Kidney stones, change in eGFR, urine oxalate, and plasma oxalate were the strongest candidate end points. Kidney stones affect how patients with primary hyperoxaluria feel and function, but standards for measurement and monitoring are lacking. Primary hyperoxaluria registry data suggest that eGFR decline in most patients is gradual, but can be unpredictable. Epidemiologic data show a strong relationship between urine oxalate and long-term kidney function loss. Urine oxalate is reasonably likely to predict clinical benefit, due to its causal role in stone formation and kidney damage in CKD stages 1-3a, and plasma oxalate is likely associated with risk of systemic oxalosis in CKD 3b-5. Change in slope of eGFR could be considered the equivalent of a clinically meaningful end point in support of traditional approval. A substantial change in urine oxalate as a surrogate end point could support traditional approval in patients with primary hyperoxaluria type 1 and CKD stages 1-3a. A substantial change in markedly elevated plasma oxalate could support accelerated approval in patients with primary hyperoxaluria and CKD stages 3b-5. Primary hyperoxaluria type 1 accounts for the preponderance of available data, thus heavily influences the conclusions. Addressing gaps in data will further facilitate testing of promising new treatments, accelerating improved outcomes for patients with primary hyperoxaluria.
Keywords: biomarkers; chronic; clinical trial end points; hyperoxaluria; kidney; kidney calculi; kidney stones; liver transplantation; oxalate; primary; primary hyperoxaluria type 1; rare kidney disease; registries; renal dialysis; renal insufficiency.
Copyright © 2020 by the American Society of Nephrology.
Figures
Comment in
-
Re: Endpoints for Clinical Trials in Primary Hyperoxaluria.J Urol. 2020 Sep;204(3):613. doi: 10.1097/JU.0000000000001173.02. Epub 2020 Jun 18. J Urol. 2020. PMID: 32552323 No abstract available.
References
-
- Cochat P, Rumsby G: Primary hyperoxaluria. N Engl J Med 369: 649–658, 2013 - PubMed
-
- Garrelfs SF, Rumsby G, Peters-Sengers H, Erger F, Groothoff J, Beck B, Oosterveld MJS, Pelle A, Neuhaus T, Adams B, Cochat P, Salido E, Lipkin GW, Hoppe B, Hulton SA; OxalEurope Consortium: Patients with Primary Hyperoxaluria type 2 have significant morbidity and require careful follow-up. Kidney Int 96: 1389–1399, 2019 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
