

PEER umbrella systematic review of systematic reviews: Management of osteoarthritis in primary care
- PMID: 32165479
- PMCID: PMC8302337
PEER umbrella systematic review of systematic reviews: Management of osteoarthritis in primary care
Abstract
Objective: To determine how many patients with chronic osteoarthritis pain respond to various non-surgical treatments.
Data sources: PubMed and the Cochrane Library.
Study selection: Published systematic reviews of randomized controlled trials (RCTs) that included meta-analysis of responder outcomes for at least 1 of the following interventions were included: acetaminophen, oral nonsteroidal anti-inflammatory drugs (NSAIDs), topical NSAIDs, serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants, cannabinoids, counseling, exercise, platelet-rich plasma, viscosupplementation, glucosamine, chondroitin, intra-articular corticosteroids, rubefacients, or opioids.
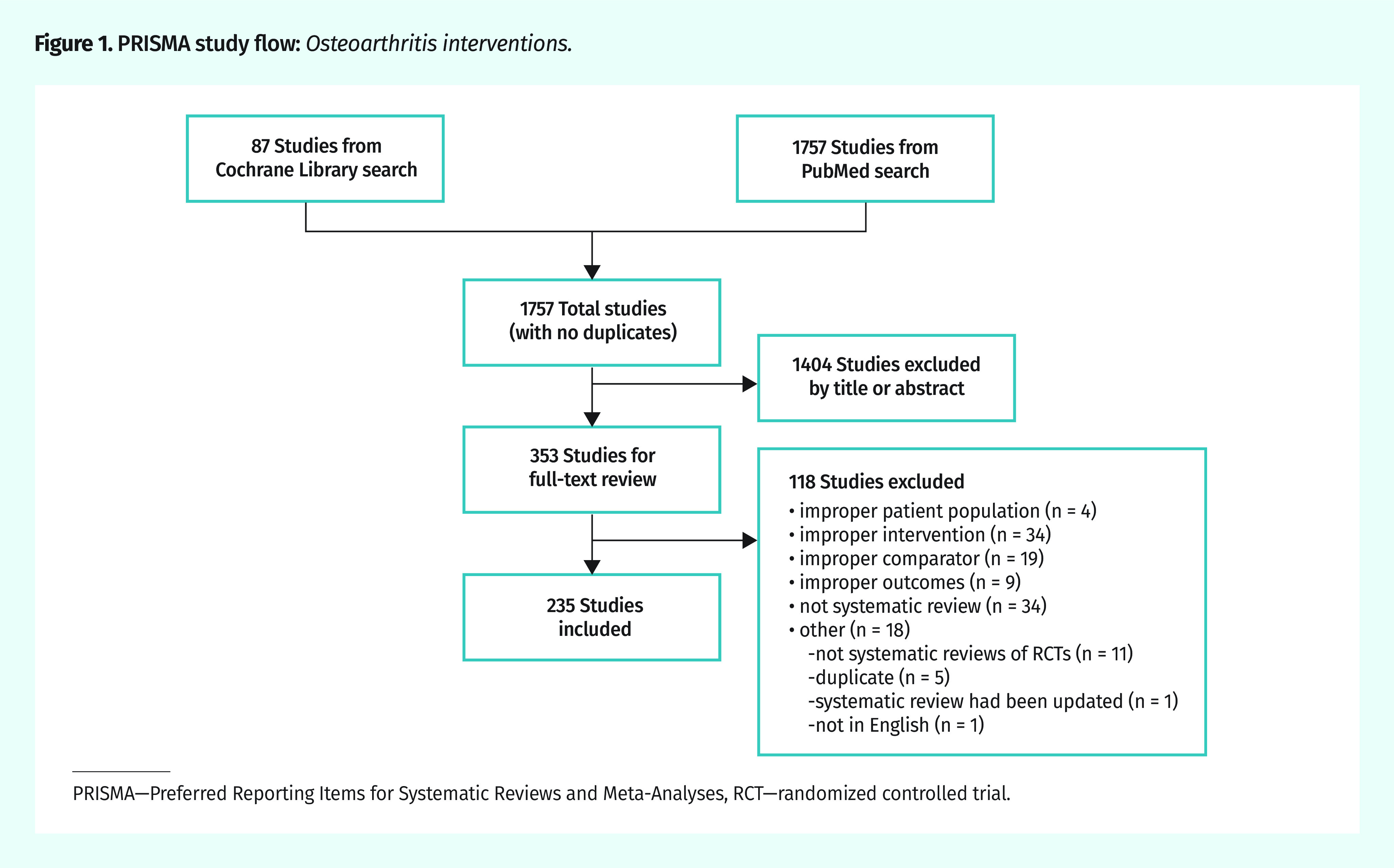
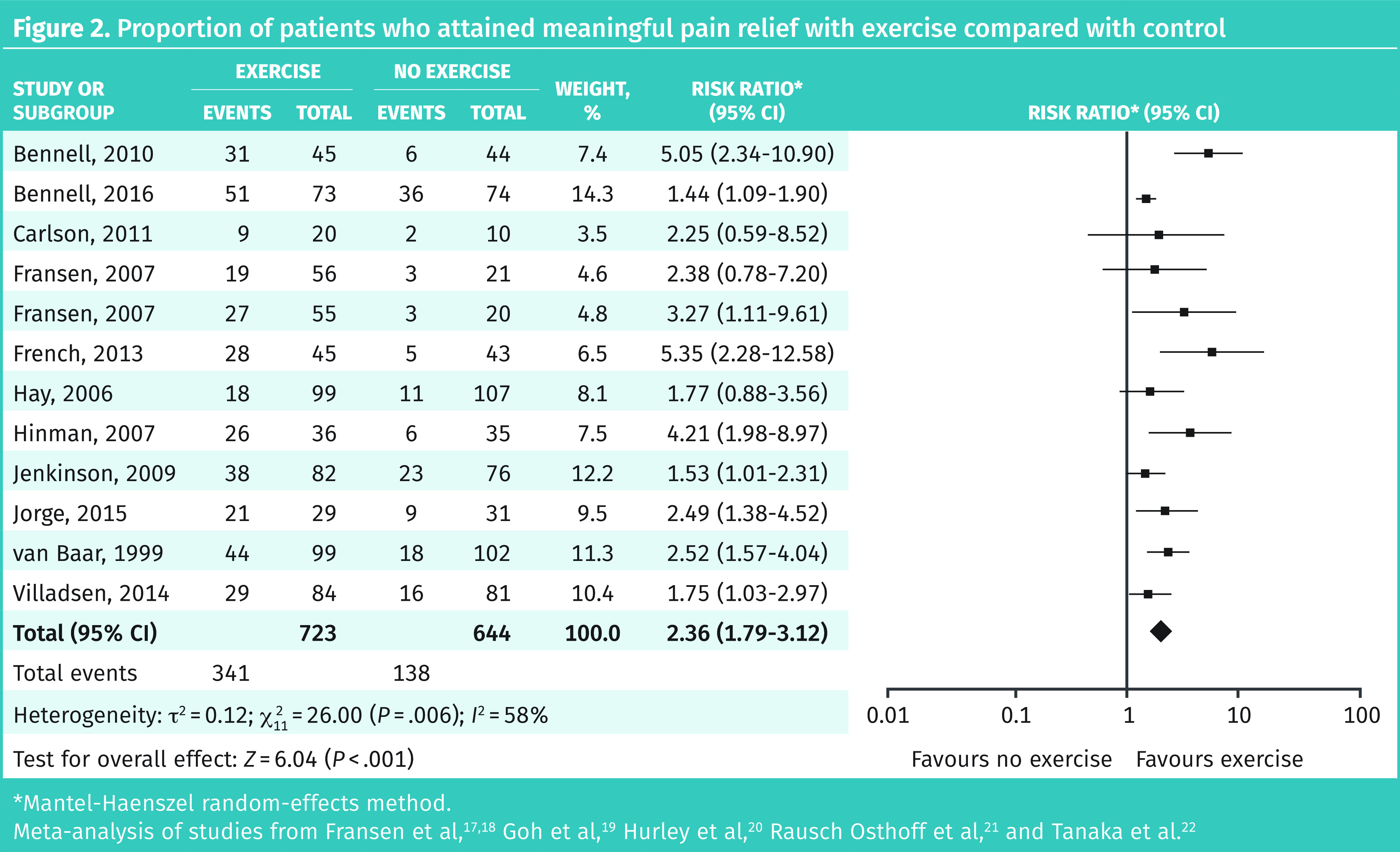
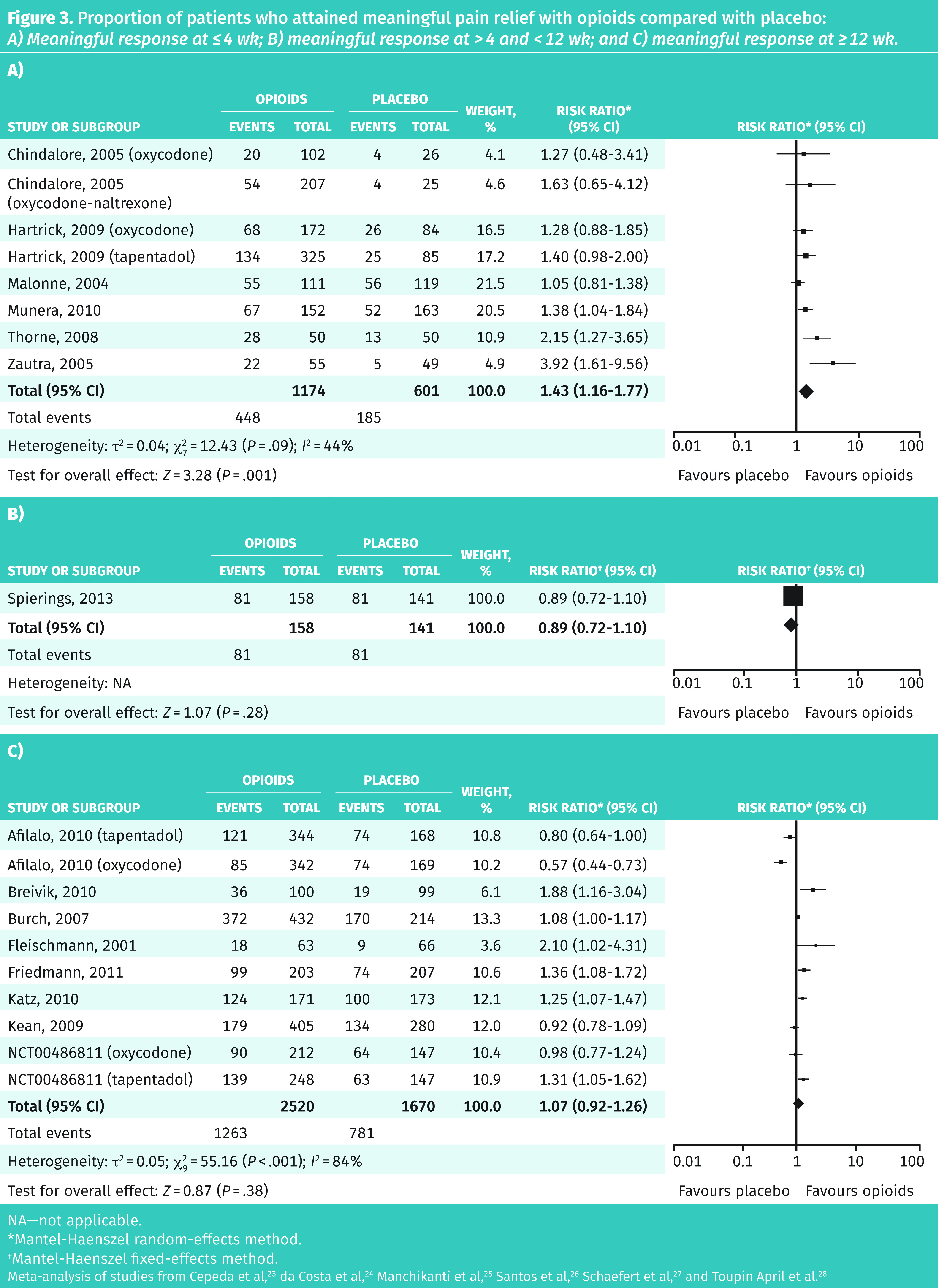
Synthesis: In total, 235 systematic reviews were included. Owing to limited reporting of responder meta-analyses, a post hoc decision was made to evaluate individual RCTs with responder analysis within the included systematic reviews. New meta-analyses were performed where possible. A total of 155 RCTs were included. Interventions that led to more patients attaining meaningful pain relief compared with control included exercise (risk ratio [RR] of 2.36; 95% CI 1.79 to 3.12), intra-articular corticosteroids (RR = 1.74; 95% CI 1.15 to 2.62), SNRIs (RR = 1.53; 95% CI 1.25 to 1.87), oral NSAIDs (RR = 1.44; 95% CI 1.36 to 1.52), glucosamine (RR = 1.33; 95% CI 1.02 to 1.74), topical NSAIDs (RR = 1.27; 95% CI 1.16 to 1.38), chondroitin (RR = 1.26; 95% CI 1.13 to 1.41), viscosupplementation (RR = 1.22; 95% CI 1.12 to 1.33), and opioids (RR = 1.16; 95% CI 1.02 to 1.32). Preplanned subgroup analysis demonstrated no effect with glucosamine, chondroitin, or viscosupplementation in studies that were only publicly funded. When trials longer than 4 weeks were analyzed, the benefits of opioids were not statistically significant.
Conclusion: Interventions that provide meaningful relief for chronic osteoarthritis pain might include exercise, intra-articular corticosteroids, SNRIs, oral and topical NSAIDs, glucosamine, chondroitin, viscosupplementation, and opioids. However, funding of studies and length of treatment are important considerations in interpreting these data.
Objectif: Déterminer le nombre de patients souffrant de douleur due à l’arthrose chronique qui répondent à divers traitements non chirurgicaux.
Qualité des données: PubMed et la bibliothèque Cochrane.
Sélection des études: Nous avons inclus les revues systématiques publiées d’études randomisées contrôlées (ERC) qui incluaient une méta-analyse des résultats chez les sujets répondants pour au moins 1 des interventions suivantes : l’acétaminophène, les anti-inflammatoires non stéroïdiens (AINS) par voie orale, les AINS topiques, les inhibiteurs de la recapture de la sérotoninenorépinéphrine (IRSN), les antidépresseurs tricycliques, les cannabinoïdes, le counseling, l’exercice, le plasma riche en plaquettes, la viscosupplémentation, la glucosamine, la chondroïtine, les corticostéroïdes intra-articulaires, les rubéfiants ou les opioïdes.
Synthèse: Au total, 235 revues systématiques ont été incluses. En raison des rapports limités des méta-analyses sur les sujets répondants, une décision a été prise a posteriori d’évaluer les ERC individuelles qui comportaient une analyse des sujets répondants parmi les revues systématiques incluses. De nouvelles méta-analyses ont été effectuées, dans la mesure du possible. Un total de 155 ERC ont été retenues. Parmi les interventions qui ont entraîné un soulagement plus significatif de la douleur chez les patients par rapport aux groupes témoins figuraient l’exercice (risque relatif [RR] = 2,36; IC à 95 % de 1,79 à 3,12), les corticostéroïdes intra-articulaires (RR = 1,74; IC à 95 % de 1,15 à 2,62), les IRSN (RR = 1,53; IC à 95 % de 1,25 à 1,87), les AINS par voie orale (RR = 1,44; IC à 95 % de 1,36 à 1,52), la glucosamine (RR = 1,33; IC à 95 % de 1,02 à 1,74), les AINS topiques (RR = 1,27; IC à 95 % de 1,16 à 1,38), la chondroïtine (RR = 1,26; IC à 95 % de 1,13 à 1,41), la viscosupplémentation (RR = 1,22; IC à 95 % de 1,12 à 1,33), et les opioïdes (RR = 1,16; IC à 95 % de 1,02 à 1,32). Une analyse planifiée de sousgroupes n’a démontré aucun effet avec la glucosamine, la chondroïtine ou la viscosupplémentation dans les études qui étaient financées seulement par le secteur public. Dans l’analyse des études d’une durée de plus de 4 semaines, les bienfaits des opioïdes n’étaient pas statistiquement significatifs.
Conclusion: Parmi les interventions qui pourraient procurer un soulagement significatif de la douleur causée par l’arthrose chronique, on peut mentionner l’exercice, les corticostéroïdes intra-articulaires, les IRSN, les AINS par voie orale et topiques, la glucosamine, la chondroïtine, la viscosupplémentation et les opioïdes. Par ailleurs, le financement des études et la durée du traitement sont des facteurs importants à considérer dans l’interprétation de ces données.
Copyright© the College of Family Physicians of Canada.
Figures
Comment in
-
Misleading communication aid.Can Fam Physician. 2020 Jun;66(6):393. Can Fam Physician. 2020. PMID: 32532715 Free PMC article. No abstract available.
-
Response.Can Fam Physician. 2020 Jun;66(6):393-396. Can Fam Physician. 2020. PMID: 32532716 Free PMC article. No abstract available.
References
-
- Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–59. - PubMed
-
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197–223. Erratum in: Lancet 2013;381(9867):628. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical