

Spine deformities in patients with cerebral palsy; the role of the pelvis
- PMID: 32165976
- PMCID: PMC7043121
- DOI: 10.1302/1863-2548.14.190141
Spine deformities in patients with cerebral palsy; the role of the pelvis
Abstract
Introduction: Progressive neuromuscular spinal deformities with pelvic obliquity and loss of sitting balance are typical features of severely affected patients with cerebral palsy. The pelvis represents the key bone between the spine and the lower extremity when it comes to deciding whether and when to operate and if spine or hip surgery first is beneficial. The pelvis can be looked at as the lowest vertebra and as the rooftop of the lower extremities.
Biomechanical considerations: To allow for a normal spinal shape, the pelvis needs to be horizontal in the frontal plane and mildly anterior tilted in the sagittal plane, less for sitting and more for standing. Any abnormal pelvic position requires spinal compensation and challenges the equilibrium control of the individual. Both anatomical neighbourhoods - the spine and the hip joints - have to be considered when spinal deformities, hip instability and contractures evolve, in conservative therapy (bracing, physiotherapy, seating in the wheelchair) and when surgical interventions are weighed out against each other.
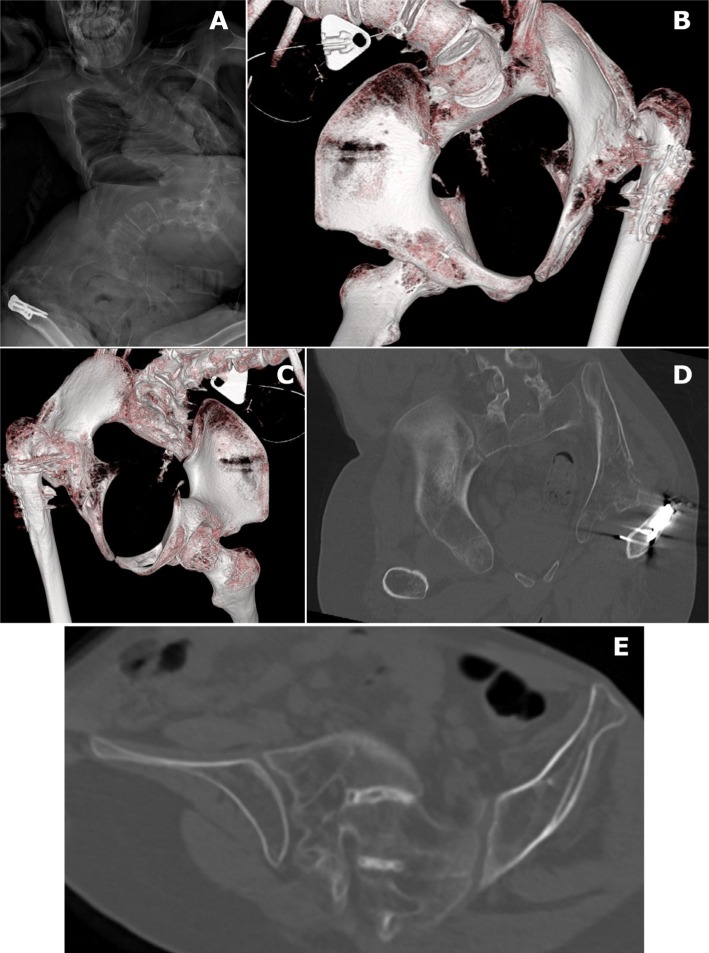
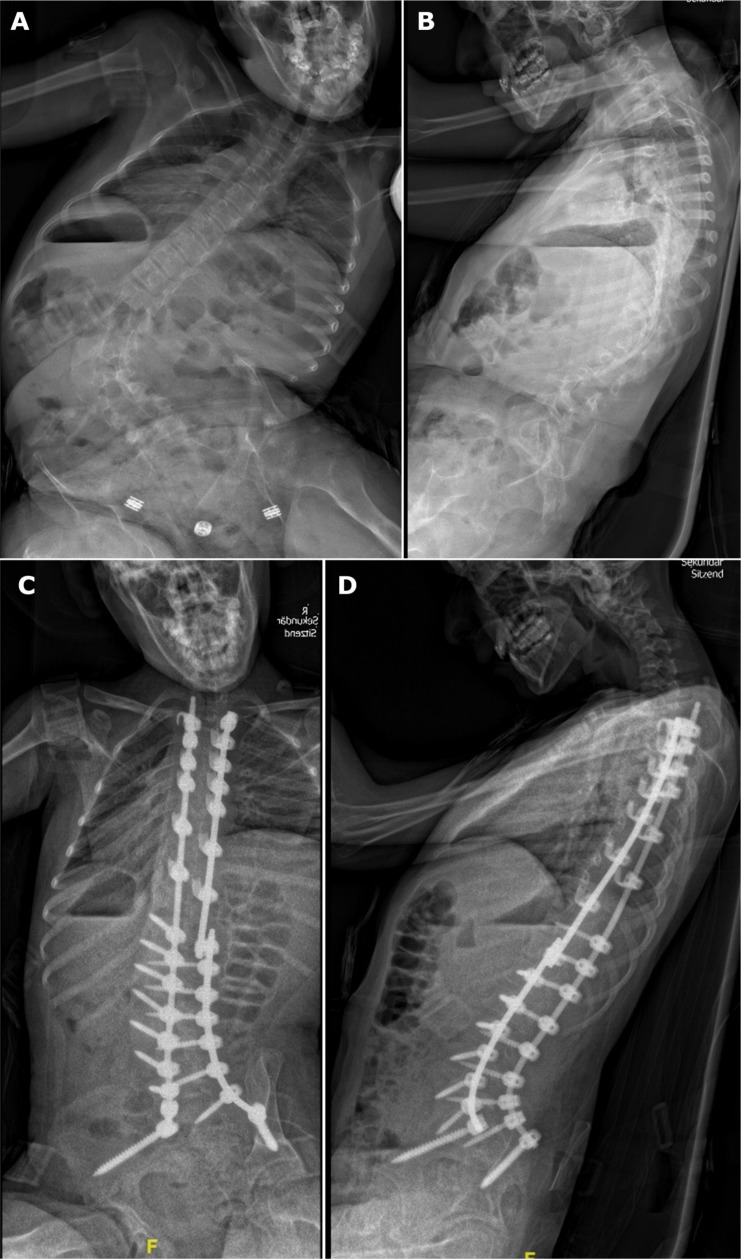
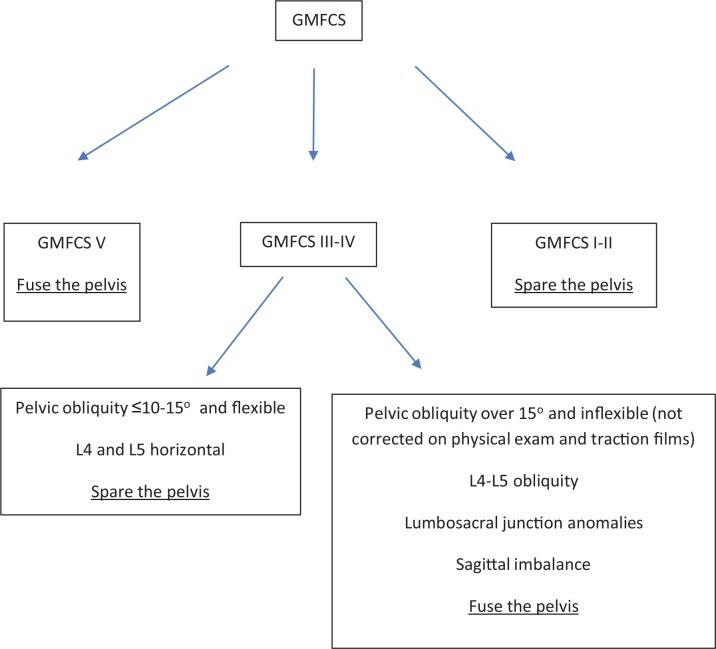
Surgical considerations: Multiple anatomical factors such as sagittal profile and pelvic orientiation, pelvic transverse plane asymmetries and lumbosacral malformations have to be considered in case the pelvis is instrumented with sacral and iliac screws. Rotational deformities and asymmetries of the pelvic bones make the safe insertion of long screws challenging. Advantages of primary pelvic fixation include correction of pelvic obliquity, especially considering the lever arm of the whole spinal construct. The risk of revision surgery due to progression of distal curves is also reduced. Disadvantages of pelvic fixation include the complexity of the additional intervention, which may result in longer operating times, increased risk of blood loss, infection and hardware malpositioning.
Keywords: cerebral palsy; deformity; pelvis; spine.
Copyright © 2020, The author(s).
Figures

References
-
- Master DL, Son-Hing JP, Poe-Kochert C, Armstrong DG, Thompson GH. Risk factors for major complications after surgery for neuromuscular scoliosis. Spine (Phila Pa 1976) 2011;36:564-571. - PubMed
-
- Yoshida K, Kajiura I, Suzuki T, Kawabata H. Natural history of scoliosis in cerebral palsy and risk factors for progression of scoliosis. J Orthop Sci 2018;23:649-652. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
