

Spinal sagittal alignment and head control in patients with cerebral palsy
- PMID: 32165977
- PMCID: PMC7043126
- DOI: 10.1302/1863-2548.14.190160
Spinal sagittal alignment and head control in patients with cerebral palsy
Abstract
Purpose: Spinal sagittal alignment restoration has been associated with improved functional outcomes and with reduced complications rates. Several limitations exist for radiological analysis in cerebral palsy (CP) patients. The goal of this study was to summarize the existing literature and report the important considerations to evaluate in a CP patient undergoing spinal surgery.
Methods: A retrospective radiological analysis was performed, including non-ambulant CP children with progressive scoliosis. Full-spine sitting radiographs performed pre-and postoperatively were required to measure spino-pelvic sagittal parameters.
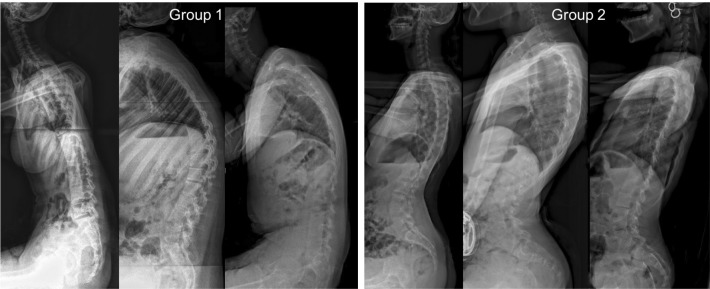
Result: A total of 23 non-ambulating CP patients were included, mean age 16.0 years (standard error of the mean 0.5). Two distinct groups of patients were identified. Group 1 (61%) were patients with less trunk control (lumbar lordosis (LL) < 50°), retroverted and vertical pelvis (mean sacral slope (SS) 11.4° and pelvic tilt (PT) 38.1°) and anterior imbalance (mean sagittal vertical axis (SVA) 5.9 cm) and Group 2 (39%) were patients with better trunk control (LL > 60°, anteverted and horizontal pelvis (mean SS 49.3°, PT 9.7°) and posterior imbalance (mean SVA 5.8 cm). Postoperative measures showed significant impact of surgery with a PT reduction of 19° (p = 0.007), a mean SS increase of 15° (p = 0.04) and a LL gained of 10° (p = 0.2).
Conclusion: Sagittal spino-pelvic alignment in non-ambulating CP patients remains difficult to assess. The current literature is poor but our radiological study was able to define two distinct groups among Gross Motor Function Classification System (GMFCS) level V patients, based on the quality of their trunk control. All possible factors that may influence head and trunk posture should be systematically considered and optimized.
Level of evidence: Level IV.
Keywords: cerebral palsy; children; non-ambulant; sagittal spinal alignment.
Copyright © 2020, The author(s).
Figures



References
-
- Schwab F, Patel A, Ungar B, Farcy J-P, Lafage V. Adult spinal deformity-postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine (Phila Pa 1976) 2010;35:2224-2231. - PubMed
-
- Ilharreborde B. Sagittal balance and idiopathic scoliosis: does final sagittal alignment influence outcomes, degeneration rate or failure rate? Eur Spine J 2018;27(suppl 1):48-58. - PubMed
-
- Suh S-W, Suh D-H, Kim J-W, Park J-H, Hong J-Y. Analysis of sagittal spinopelvic parameters in cerebral palsy. Spine J 2013;13:882-888. - PubMed
-
- Kim Y, Moon ES, Park JO, et al. The thoracic lordosis correction improves sacral slope and walking ability in neuromuscular scoliosis. Clin Spine Surg 2016;29:E413-E420. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
