

Increasing Cardiovascular Data Sampling Frequency and Referencing It to Baseline Improve Hemorrhage Detection
- PMID: 32166238
- PMCID: PMC7063895
- DOI: 10.1097/CCE.0000000000000058
Increasing Cardiovascular Data Sampling Frequency and Referencing It to Baseline Improve Hemorrhage Detection
Abstract
We hypothesize that knowledge of a stable personalized baseline state and increased data sampling frequency would markedly improve the ability to detect progressive hypovolemia during hemorrhage earlier and with a lower false positive rate than when using less granular data.
Design: Prospective temporal challenge.
Setting: Large animal research laboratory, University Medical Center.
Subjects: Fifty-one anesthetized Yorkshire pigs.
Interventions: Pigs were instrumented with arterial, pulmonary arterial, and central venous catheters and allowed to stabilize for 30 minutes then bled at a constant rate of either 5 mL·min-1 (n = 13) or 20 (n = 38) until mean arterial pressure decreased to 40 or 30 mm Hg in the 5 and 20 mL·min-1 pigs, respectively.
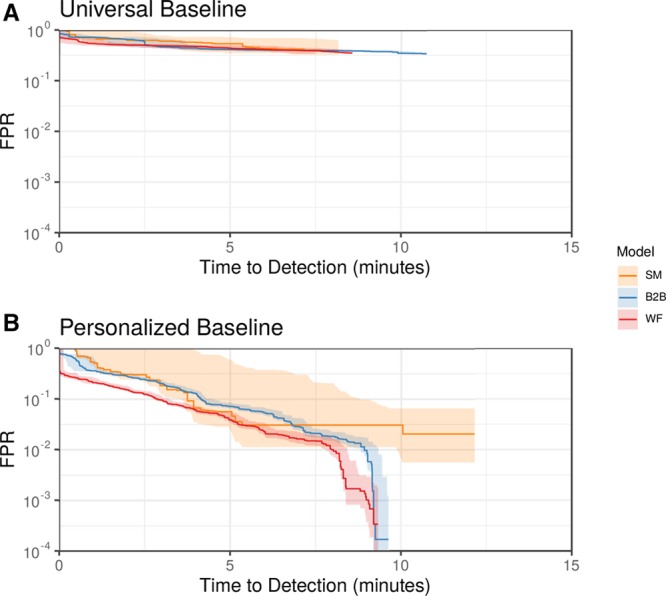
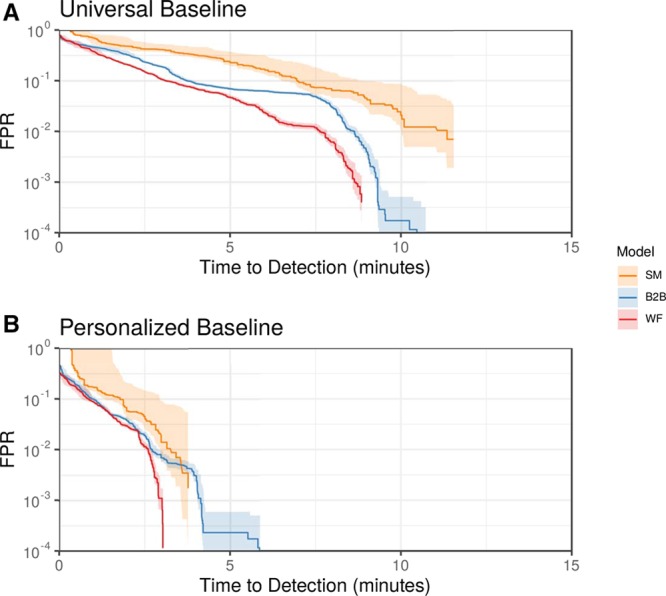
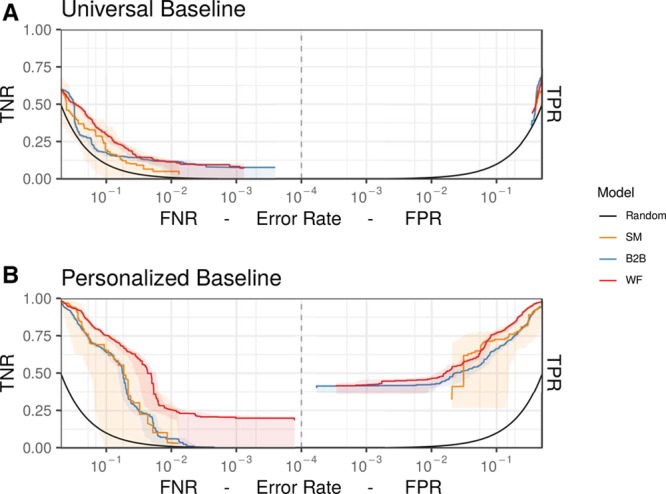
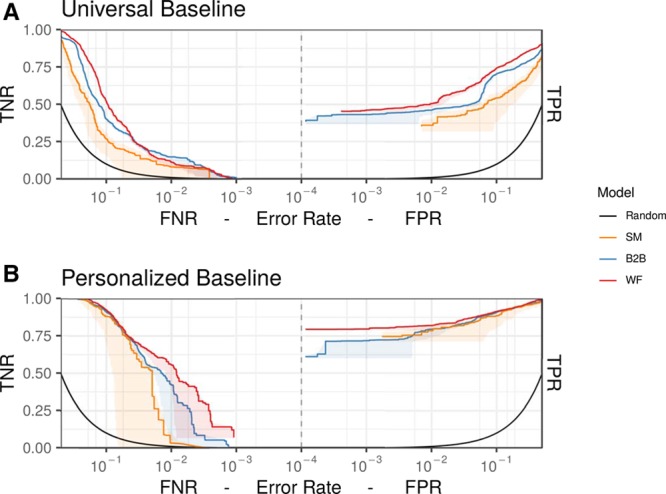
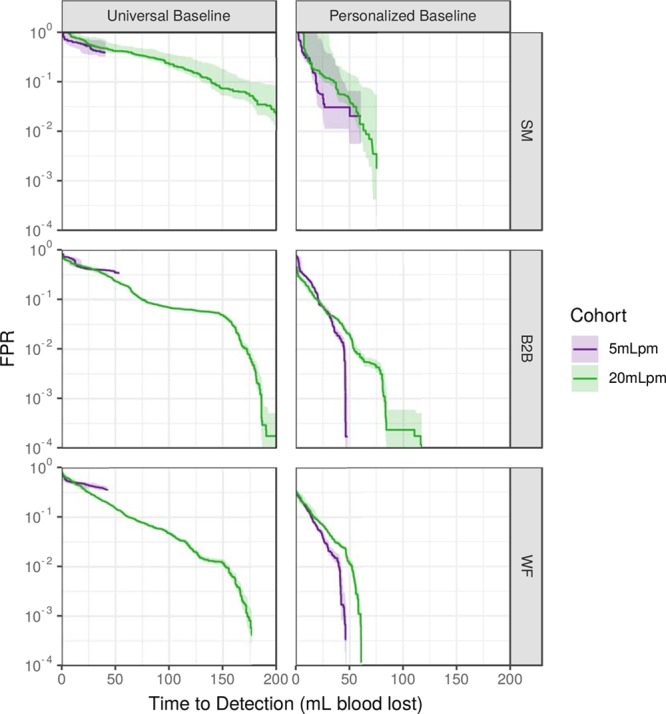
Measurements and main results: Data during the stabilization period served as baseline. Hemodynamic variables collected at 250 Hz were used to create predictive models of "bleeding" using featurized beat-to-beat and waveform data and compared with models using mean unfeaturized hemodynamic variables averaged over 1-minute as simple hemodynamic metrics using random forest classifiers to identify bleeding with or without baseline data. The robustness of the prediction was evaluated in a leave-one-pig-out cross-validation. Predictive performance of models was compared by their activity monitoring operating characteristic and receiver operating characteristic profiles. Primary hemodynamic threshold data poorly identified bleed onset unless very stable initial baseline reference data were available. When referenced to baseline, bleed detection at a false positive rates of 10-2 with time to detect 80% of pigs bleeding was similar for simple hemodynamic metrics, beat-to-beat, and waveform at about 3-4 minutes. Whereas when universally baselined, increasing sampling frequency reduced latency of bleed detection from 10 to 8 to 6 minutes, for simple hemodynamic metrics, beat-to-beat, and waveform, respectively. Some informative features differed between simple hemodynamic metrics, beat-to-beat, and waveform models.
Conclusions: Knowledge of personal stable baseline data allows for early detection of new-onset bleeding, whereas if no personal baseline exists increasing sampling frequency of hemodynamic monitoring data improves bleeding detection earlier and with lower false positive rate.
Keywords: animal model; hemodynamic monitoring; hemorrhage; machine learning; predictive models.
Copyright © 2019 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
Similar articles
-
Parsimony of Hemodynamic Monitoring Data Sufficient for the Detection of Hemorrhage.Anesth Analg. 2020 May;130(5):1176-1187. doi: 10.1213/ANE.0000000000004564. Anesth Analg. 2020. PMID: 32287125 Free PMC article.
-
The CNAP™ Finger Cuff for Noninvasive Beat-To-Beat Monitoring of Arterial Blood Pressure: An Evaluation in Intensive Care Unit Patients and a Comparison with 2 Intermittent Devices.Anesth Analg. 2016 Nov;123(5):1126-1135. doi: 10.1213/ANE.0000000000001324. Anesth Analg. 2016. PMID: 27159068
-
Tracking central hypovolemia with ecg in humans: cautions for the use of heart period variability in patient monitoring.Shock. 2010 Jun;33(6):583-9. doi: 10.1097/SHK.0b013e3181cd8cbe. Shock. 2010. PMID: 19997052
-
Continuous fiberoptic arterial and venous blood gas monitoring in hemorrhagic shock.Chest. 1996 Apr;109(4):1049-55. doi: 10.1378/chest.109.4.1049. Chest. 1996. PMID: 8635330
-
Lithium dilution measurement of cardiac output and arterial pulse waveform analysis: an indicator dilution calibrated beat-by-beat system for continuous estimation of cardiac output.Curr Opin Crit Care. 2002 Jun;8(3):257-61. doi: 10.1097/00075198-200206000-00010. Curr Opin Crit Care. 2002. PMID: 12386506 Review.
Cited by
-
Automated Assessment of Cardiovascular Sufficiency Using Non-Invasive Physiological Data.Sensors (Basel). 2022 Jan 28;22(3):1024. doi: 10.3390/s22031024. Sensors (Basel). 2022. PMID: 35161770 Free PMC article.
-
Continuous ECG monitoring should be the heart of bedside AI-based predictive analytics monitoring for early detection of clinical deterioration.J Electrocardiol. 2023 Jan-Feb;76:35-38. doi: 10.1016/j.jelectrocard.2022.10.011. Epub 2022 Nov 2. J Electrocardiol. 2023. PMID: 36434848 Free PMC article. Review.
-
Development of hemorrhage identification model using non-invasive vital signs.Physiol Meas. 2020 Jun 10;41(5):055010. doi: 10.1088/1361-6579/ab8cb2. Physiol Meas. 2020. PMID: 32325439 Free PMC article.
-
Early Physiologic Numerical and Waveform Characteristics of Simulated Hemorrhagic Events With Healthy Volunteers Donating Blood.Crit Care Explor. 2024 Mar 26;6(4):e1073. doi: 10.1097/CCE.0000000000001073. eCollection 2024 Apr. Crit Care Explor. 2024. PMID: 38545607 Free PMC article.
-
Intelligent Clinical Decision Support.Sensors (Basel). 2022 Feb 12;22(4):1408. doi: 10.3390/s22041408. Sensors (Basel). 2022. PMID: 35214310 Free PMC article.
References
-
- Kauvar DS, Lefering R, Wade CE. Impact of hemorrhage on trauma outcome: An overview of epidemiology, clinical presentations, and therapeutic considerations. J Trauma 200660S3–S11 - PubMed
-
- Calzavacca P, Licari E, Tee A, et al. A prospective study of factors influencing the outcome of patients after a medical emergency team review. Intensive Care Med 2008342112–2116 - PubMed
-
- McNicholl BP. The golden hour and prehospital trauma care. Injury 199425251–254 - PubMed
-
- Norris PR, Morris JA, Jr, Ozdas A, et al. Heart rate variability predicts trauma patient outcome as early as 12 h: Implications for military and civilian triage. J Surg Res 2005129122–128 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
