

Mortality Prediction in Rural Kenya: A Cohort Study of Mechanical Ventilation in Critically Ill Patients
- PMID: 32166248
- PMCID: PMC7063927
- DOI: 10.1097/CCE.0000000000000067
Mortality Prediction in Rural Kenya: A Cohort Study of Mechanical Ventilation in Critically Ill Patients
Abstract
Critical care is expanding in low- and middle-income countries. Yet, due to factors such as missing data and different disease patterns, predictive scores often fail to adequately predict the high rates of mortality observed.
Objectives: We evaluated multiple prognostic models for the outcome of mortality in critically ill, mechanically ventilated patients in rural Kenya and examined factors contributing to mortality in our setting.
Design setting and participants: A prospective cohort study was conducted on mechanically ventilated patients in rural Kenya. Consecutive patients 16 years old and older initiated on mechanical ventilation between January 1, 2016, and April 30, 2017, at Tenwek Hospital were included. Demographic data, clinical characteristics, and patient outcomes were collected during routine clinical care.
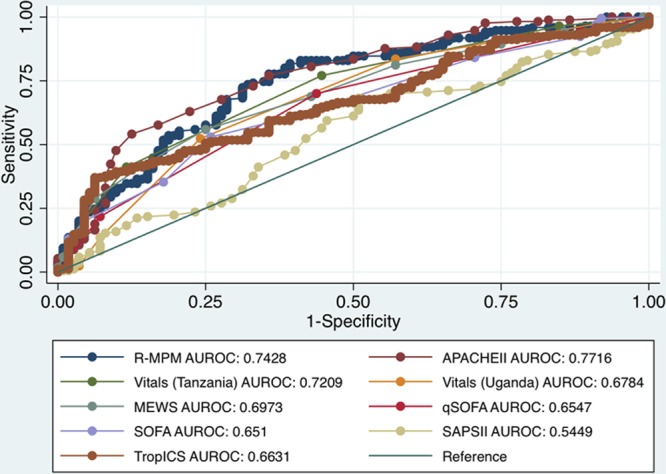
Main outcomes and measures: We assessed the discrimination and calibration of multiple previously-described models for mortality: Acute Physiology and Chronic Health Evaluation II, Sequential Organ Failure Assessment, quick Sequential Organ Failure Assessment, Simplified Acute Physiology Score II, Modified Early Warning Score, Tropical Intensive Care Score, Rwanda-Mortality Predictive Model, Vitals score (validated in Tanzania), and Vitals score for sepsis (validated in Uganda). Factors most associated with mortality were analyzed in our cohort utilizing stepwise regression.
Results: Among the final cohort of 300 patients, the overall mortality rate was 60.7%, the average age was 39.9 years, 65% were male, and 33% were seen at an outside facility prior to admission to the critical care unit. Missing variables occurred in patients for numerous models but were complete in most adapted to resource-limited settings. Models displayed moderate prediction of mortality and variable discrimination area under the receiver operating characteristic curves (and Hosmer-Lemeshow chi-square statistic) of 0.77 (22.4) for Acute Physiology and Chronic Health Evaluation II, 0.70 (3.4) for Modified Early Warning Score, 0.65 (0.16) for quick Sequential Organ Failure Assessment, 0.55 (18.4) for Simplified Acute Physiology Score II and 0.74 (9.2) for Rwanda-Mortality Predictive Model, 0.72 (0.12) for Vitals Tanzania, 0.68 (14.7) for Vitals Uganda, and 0.65 (13.9) for Tropical Intensive Care Score. Variables associated with increased mortality in our population were hypotension, infection, traumatic brain injury, and hematocrit.
Conclusions and relevance: Overall, survival for critically ill patients in rural Kenya was poor, but predictable with contributing factors. Models designed for resource-constrained settings had favorable discrimination and better calibration for mortality prediction than high-resource models in our population of mechanically ventilated, critically ill patients in rural Kenya.
Keywords: artificial; country; critical care; developing; health resource; models; respiration; statistical.
Copyright © 2019 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Stafford RE, Morrison CA, Godfrey G, et al. Challenges to the provision of emergency services and critical care in resource-constrained settings. Glob Heart 20149319–323 - PubMed
-
- Pisani L, Algera AG, Serpa Neto A, et al. ; PRoVENT–iMIC investigators, MORU and the PROVE network PRactice of VENTilation in Middle-Income Countries (PRoVENT-iMIC): Rationale and protocol for a prospective international multicentre observational study in intensive care units in Asia. BMJ Open 20188e020841 - PMC - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
