

Implementation of an ICU Recovery Clinic at a Tertiary Care Academic Center
- PMID: 32166275
- PMCID: PMC7063951
- DOI: 10.1097/CCE.0000000000000034
Implementation of an ICU Recovery Clinic at a Tertiary Care Academic Center
Abstract
Post-ICU clinics may facilitate the care of survivors of critical illness, but there is a paucity of data describing post-ICU clinic implementation. We sought to describe implementation of our ICU recovery clinic, including an assessment of barriers and facilitators to clinic attendance.
Design: Adults admitted to the medical ICU of a large tertiary care academic hospital with shock and/or respiratory failure requiring mechanical ventilation were screened for participation in a newly formed ICU recovery clinic. Participant selection and attendance rates were tracked. Reasons for nonattendance were assessed by phone call in a subset of patients.
Setting: A newly formed ICU recovery clinic of a large tertiary care academic hospital.
Patients: All patients admitted to the medical ICU were screened.
Interventions: ICU recovery clinic appointments were scheduled for all eligible patients. A subset of nonattenders were called to assess reasons for nonattendance.
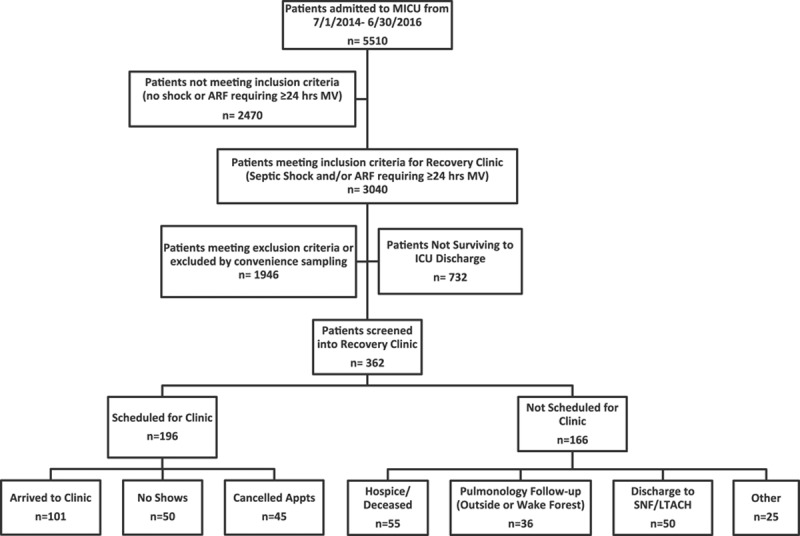
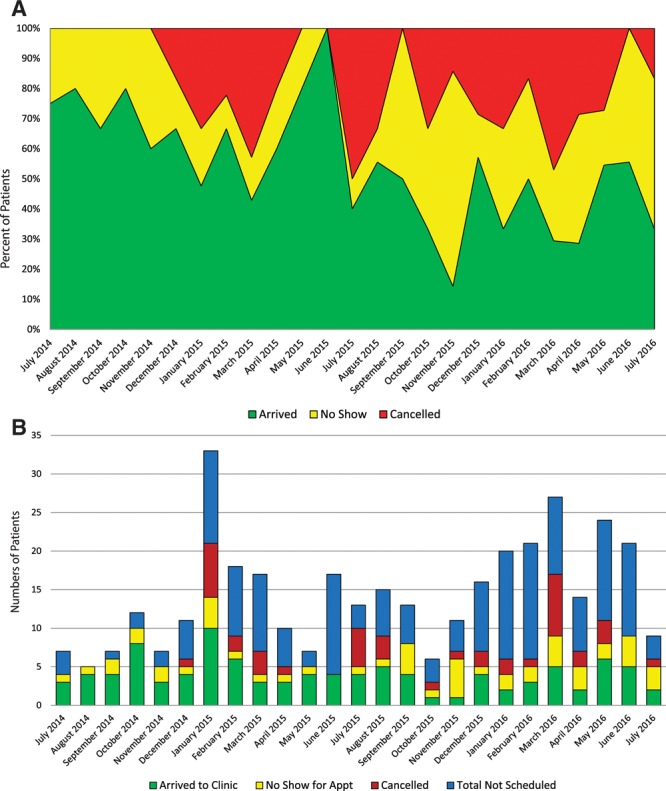
Measurements and main results: Over 2 years, we admitted 5,510 patients to our medical ICU. Three hundred sixty-two were screened into the recovery clinic. One-hundred sixty-six were not scheduled for clinic; major reasons included discharge to hospice/death in the hospital (n = 55) and discharge to a facility (n = 50). One-hundred ninety-six patients were scheduled for a visit and of those, 101 (52%) arrived to clinic. Reasons for nonattendance in a surveyed subset of nonattenders included patient's lack of awareness of the appointment (50%, n = 9/18), financial concerns (17%, n = 3/18), and transportation difficulty (17%, n = 3/18).
Conclusions: ICU recovery clinics may address the needs of survivors of critical illness. Barriers to clinic attendance include high mortality rates, high rates of clinic appointment cancelations and nonattendance, and discharge to locations such as skilled nursing facilities or long-term acute care hospitals. Improved communication to patients about the role of the clinic may facilitate attendance and minimize canceled appointments.
Keywords: acute respiratory distress syndrome; attendance; clinic; critical illness; nonattendance; sepsis.
Copyright © 2019 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Carson SS, Cox CE, Holmes GM, et al. The changing epidemiology of mechanical ventilation: A population-based study. J Intensive Care Med 200621173–182 - PubMed
-
- Needham DM, Bronskill SE, Calinawan JR, et al. Projected incidence of mechanical ventilation in Ontario to 2026: Preparing for the aging baby boomers. Crit Care Med 200533574–579 - PubMed
-
- Martin GS, Mannino DM, Eaton S, et al. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med 20033481546–1554 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
