

Initiation and Assessment of Timekeeping Roles During In-Hospital Cardiac Arrests to Track Rhythm Checks and Epinephrine Dosing
- PMID: 32166289
- PMCID: PMC7063905
- DOI: 10.1097/CCE.0000000000000069
Initiation and Assessment of Timekeeping Roles During In-Hospital Cardiac Arrests to Track Rhythm Checks and Epinephrine Dosing
Abstract
Objectives: Compliance to advanced cardiac life support algorithm is low and associated with worse outcomes from in-hospital cardiac arrests. This study aims to improve algorithm compliance by delegation of two separate code team members for timing rhythm check and epinephrine administration in accordance to the advanced cardiac life support algorithm.
Design: Prospective intervention with historical controls.
Setting: Single academic medical center.
Patients: Patients who suffered in-hospital cardiac arrest during study period were considered for inclusion. Patients in which the advanced cardiac life support algorithm or new timekeeper roles were not used were excluded.
Interventions: Two existing code team members were delegated to time epinephrine and rhythm checks.
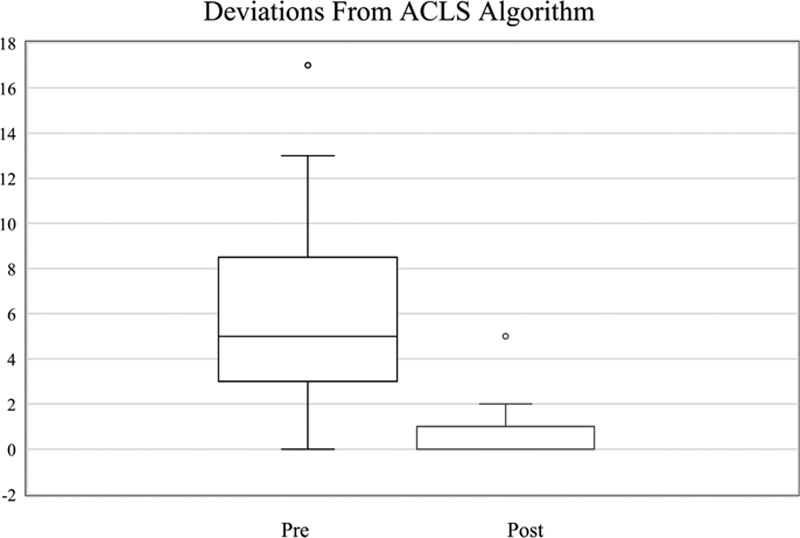
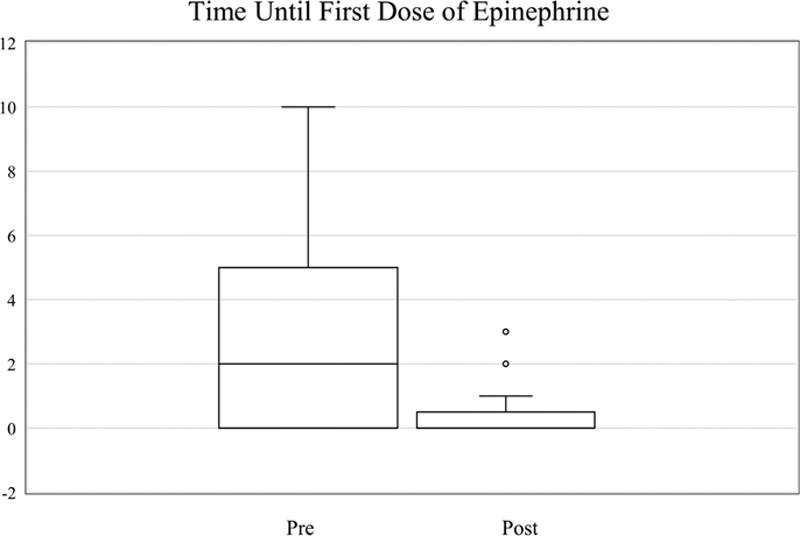
Measurements and main results: Primary endpoint was deviations from the 2-minute rhythm check or 3- to 5-minute epinephrine administration. Each deviation outside allotted time intervals was counted as one deviation. However, instances in which multiple intervals passed were counted as multiple deviations. Algorithm adherence was analyzed before and after intervention. Secondary endpoints included return of spontaneous circulation rate, time until first dose of epinephrine, and anonymous survey data. Thirteen pre intervention in-hospital cardiac arrests were compared with 13 in-hospital cardiac arrests post. Prior to intervention, the median deviation per in-hospital cardiac arrest was 5 (interquartile range, 3-7) versus 1 post (interquartile range 0-1; p = 0.0003). The median time until first dose of epinephrine was administered pre intervention was 5 minutes (interquartile range, 0-4) versus post intervention median of 0 (interquartile range, 0-0; p = 0.02). Pre-intervention return of spontaneous circulation rate was 46.1% versus 69.2% post. Surveys demonstrated advanced cardiac life support providers felt time keeping roles made it easier to track epinephrine administration and rhythm checks and improved team communication.
Conclusions: Two separate timekeeper roles during in-hospital cardiac arrests improved algorithm compliance, code team function, and was favored by code team members. Timekeeper roles may be associated with improved rates of return of spontaneous circulation and less time until the first dose of epinephrine was administered. This study is limited by small sample size and single-center design.
Keywords: advanced cardiac life support; cardiac arrest; cardiopulmonary resuscitation; epinephrine; guideline; in-hospital cardiac arrest; sudden.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Sandroni C, Nolan J, Cavallaro F, et al. In-hospital cardiac arrest: Incidence, prognosis and possible measures to improve survival. Intensive Care Med. 2007; 33:237–245 - PubMed
-
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: A report of 14720 cardiac arrests from the national registry of cardiopulmonary resuscitation. Resuscitation. 2003; 58:297–308 - PubMed
-
- Honarmand K, Mepham C, Ainsworth C, et al. Adherence to advanced cardiovascular life support (ACLS) guidelines during in-hospital cardiac arrest is associated with improved outcomes. Resuscitation. 2018; 129:76–81 - PubMed
-
- Cline DM, Welch KJ, Cline LS, et al. Physician compliance with advanced cardiac life support guidelines. Ann Emerg Med. 1995; 25:52–57 - PubMed
LinkOut - more resources
Full Text Sources
