

A Bayesian adaptive randomized phase II multicenter trial of bevacizumab with or without vorinostat in adults with recurrent glioblastoma
- PMID: 32166308
- PMCID: PMC7686463
- DOI: 10.1093/neuonc/noaa062
A Bayesian adaptive randomized phase II multicenter trial of bevacizumab with or without vorinostat in adults with recurrent glioblastoma
Abstract
Background: Bevacizumab has promising activity against recurrent glioblastoma (GBM). However, acquired resistance to this agent results in tumor recurrence. We hypothesized that vorinostat, a histone deacetylase (HDAC) inhibitor with anti-angiogenic effects, would prevent acquired resistance to bevacizumab.
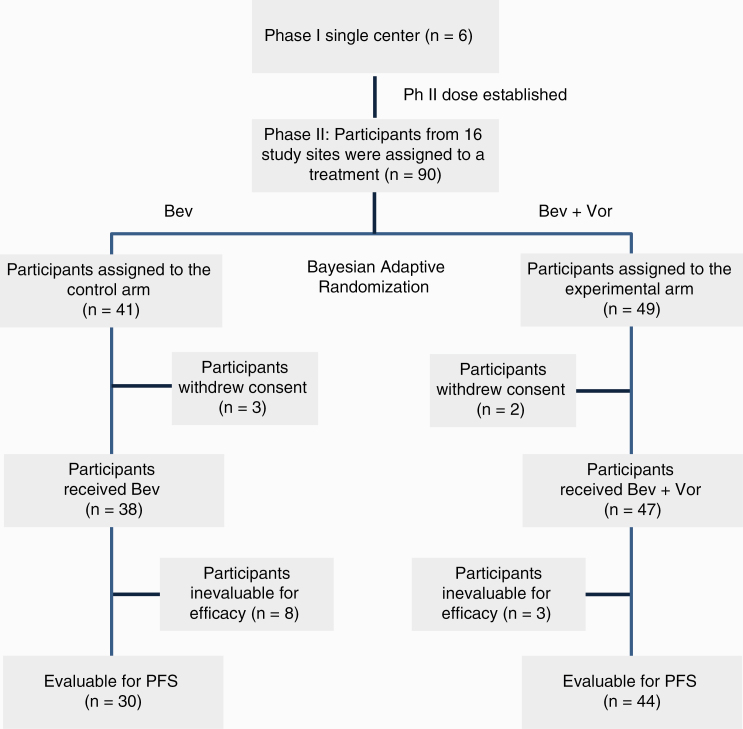
Methods: This multicenter phase II trial used a Bayesian adaptive design to randomize patients with recurrent GBM to bevacizumab alone or bevacizumab plus vorinostat with the primary endpoint of progression-free survival (PFS) and secondary endpoints of overall survival (OS) and clinical outcomes assessment (MD Anderson Symptom Inventory Brain Tumor module [MDASI-BT]). Eligible patients were adults (≥18 y) with histologically confirmed GBM recurrent after prior radiation therapy, with adequate organ function, KPS ≥60, and no prior bevacizumab or HDAC inhibitors.
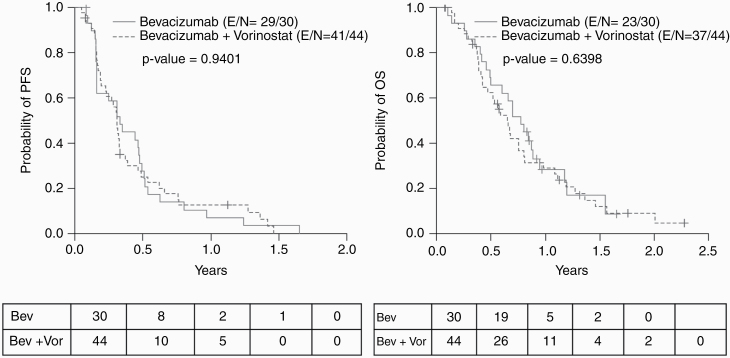
Results: Ninety patients (bevacizumab + vorinostat: 49, bevacizumab: 41) were enrolled, of whom 74 were evaluable for PFS (bevacizumab + vorinostat: 44, bevacizumab: 30). Median PFS (3.7 vs 3.9 mo, P = 0.94, hazard ratio [HR] 0.63 [95% CI: 0.38, 1.06, P = 0.08]), median OS (7.8 vs 9.3 mo, P = 0.64, HR 0.93 [95% CI: 0.5, 1.6, P = 0.79]) and clinical benefit were similar between the 2 arms. Toxicity (grade ≥3) in 85 evaluable patients included hypertension (n = 37), neurological changes (n = 2), anorexia (n = 2), infections (n = 9), wound dehiscence (n = 2), deep vein thrombosis/pulmonary embolism (n = 2), and colonic perforation (n = 1).
Conclusions: Bevacizumab combined with vorinostat did not yield improvement in PFS or OS or clinical benefit compared with bevacizumab alone or a clinical benefit in adults with recurrent GBM. This trial is the first to test a Bayesian adaptive design with adaptive randomization and Bayesian continuous monitoring in patients with primary brain tumor and demonstrates the feasibility of using complex Bayesian adaptive design in a multicenter setting.
Keywords: Bayesian adaptive trial design; bevacizumab; progression free survival; recurrent glioblastoma; vorinostat.
© The Author(s) 2020. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Cohen MH, Shen YL, Keegan P, Pazdur R. FDA drug approval summary: bevacizumab (Avastin) as treatment of recurrent glioblastoma multiforme. Oncologist. 2009;14(11):1131–1138. - PubMed
-
- Lombardi G, Pambuku A, Bellu L, et al. Effectiveness of antiangiogenic drugs in glioblastoma patients: a systematic review and meta-analysis of randomized clinical trials. Crit Rev Oncol Hematol. 2017;111:94–102. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
