

Comprehensive tumor profiling reveals unique molecular differences between peritoneal metastases and primary colorectal adenocarcinoma
- PMID: 32166754
- PMCID: PMC7505122
- DOI: 10.1002/jso.25899
Comprehensive tumor profiling reveals unique molecular differences between peritoneal metastases and primary colorectal adenocarcinoma
Abstract
Background and objectives: Peritoneal metastases (PM) from primary colorectal cancer (pCRC) are associated with poor outcomes; however, molecular differences are not well defined.
Methods: We compared unpaired tumor profiles of patients with pCRC and PM from Caris Life Sciences. Testing included next-generation sequencing of 592 genes, microsatellite instability (MSI) and tumor mutational burden (TMB). Mutations were test-defined as pathogenic (PATH).
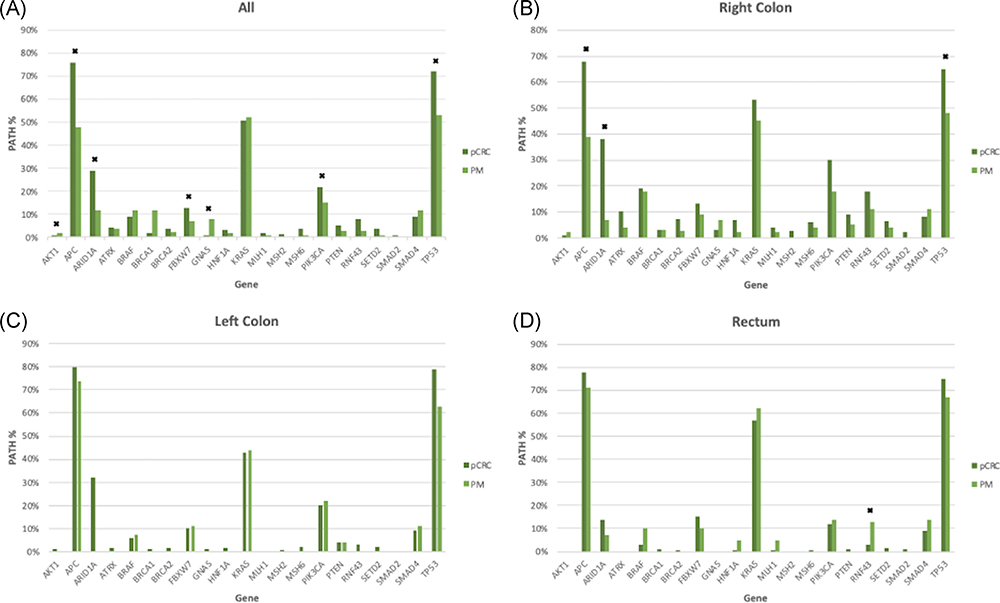
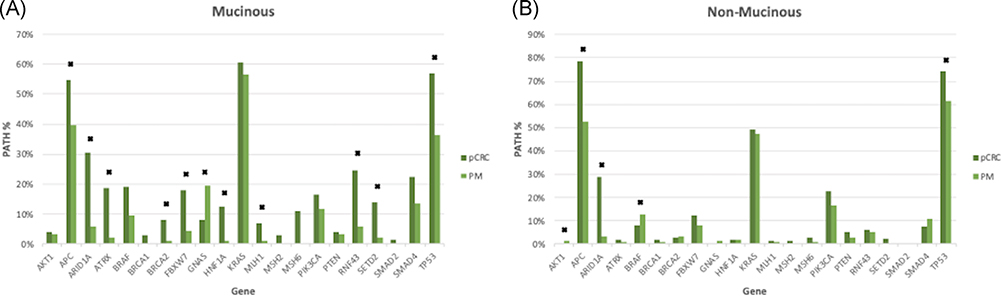
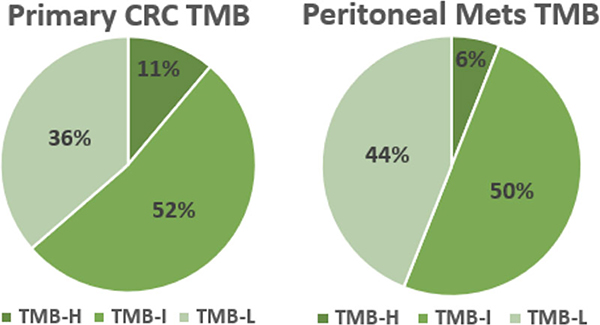
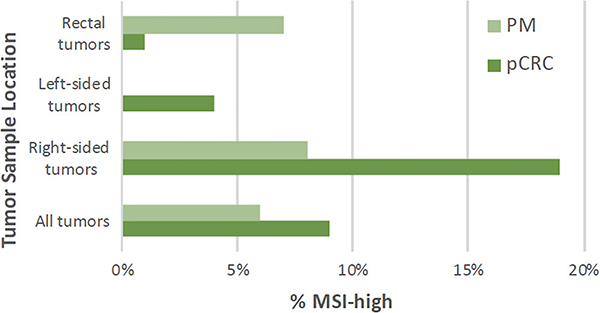
Results: Six hundred seventeen pCRC and 348 PM patients had similar gender (55% male) and age (median 59). PATHs were similar between PM and pCRC in KRAS, BRAF, SMAD2, SMAD4, and PTEN. pCRC PATHs were increased in APC (76% vs 48%, P < .01), ARID1A (29% vs 12%, P < .05), TP53 (72% vs 53%, P < .01), PIK3CA (22% vs 15%, P < .05), and FBXW7 (13% vs 7%, P < .01) compared with PM. Mucinous PM had more PATHs in GNAS (19% vs 8%, P = .032) while nonmucinous PM had more PATHs in BRAF (13% vs 8%, P = .027). Right-sided PM had decreased PATHs in APC (39% vs 68%, P < .0001), ARID1A (7% vs 38%, P < .004), and TP53 (48% vs 65%, P = .033) while there were no difference for left-sided PM. Nine percent of pCRC and 6% of PM were MSI-high (P = NS). There was no difference in TMB-high, TMB-intermediate, or TMB-low between PM and pCRC.
Conclusions: PM have similar rates of KRAS mutation with increased PATHs in GNAS (mucinous) and BRAF (nonmucinous) compared to pCRC. No differences in MSI or TMB were identified between PM and pCRC tumors. These findings inform future study into the molecular profile of PM.
Keywords: BRAF; GNAS; KRAS; carcinomatosis; colon; molecular profile.
© 2020 Wiley Periodicals, Inc.
Conflict of interest statement
CONFLICT OF INTERESTS
Dr Xiu and Dr Korn are employed by Caris Life Sciences. Dr Marshall is a consultant for Caris Life Sciences. The other authors declare that there are no conflict of interests. The content is solely the responsibility of the authors.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7–30. - PubMed
-
- Fong Y, Cohen AM, Fortner JG, et al. Liver resection for colorectal metastases. J Clin Oncol. 1997;15:938–946. - PubMed
-
- Dawson LE, Russell AH, Tong D, Wisbeck WM. Adenocarcinoma of the sigmoid colon: sites of initial dissemination and clinical patterns of recurrence following surgery alone. J Surg Oncol. 1983;22:95–99. - PubMed
-
- Russell AH, Tong D, Dawson LE, et al. Adenocarcinoma of the retroperitoneal ascending and descending colon: sites of initial dissemination and clinical patterns of recurrence following surgery alone. Int J Radiat Oncol Biol Phys. 1983;9:361–365. - PubMed
-
- Chu DZJ, Lang NP, Thompson C, Osteen PK, Westbrook KC. Peritoneal carcinomatosis in nongynecologic malignancy. A prospective study of prognostic factors. Cancer. 1989;63:364–367. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
