

Evolving surgical management of pediatric vesicoureteral reflux: is open ureteral reimplantation still the 'Gold Standard'?
- PMID: 32167694
- PMCID: PMC7088498
- DOI: 10.1590/S1677-5538.IBJU.2020.99.05
Evolving surgical management of pediatric vesicoureteral reflux: is open ureteral reimplantation still the 'Gold Standard'?
Abstract
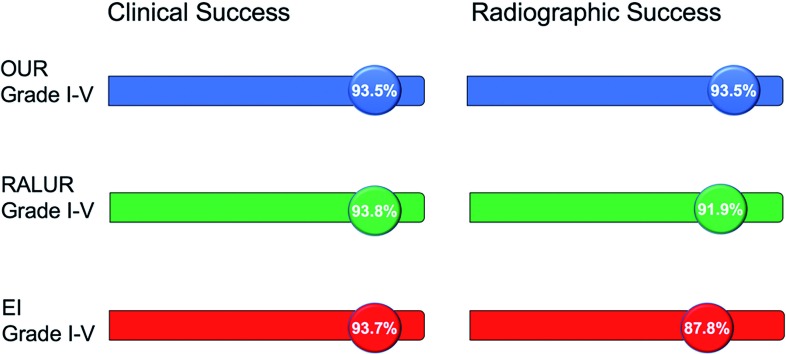
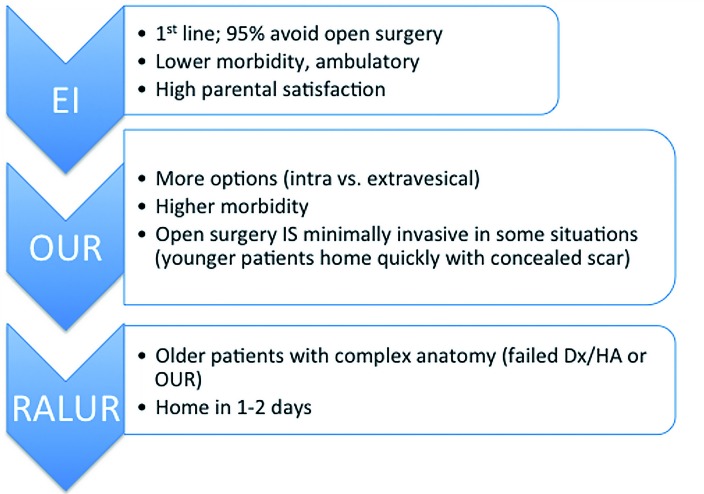
Vesicoureteral reflux, the retrograde flow of urine from the bladder into the upper urinary tract, is one of the most common urologic diagnoses in the pediatric population. Once detected, therapeutic options for urinary reflux are diverse, ranging from observation with or without continuous low-dose prophylactic antibiotics to a variety of operative interventions. While a standardized algorithm is lacking, it is generally accepted that management be tailored to individual patients based on various factors including age, likelihood of spontaneous resolution, risk of subsequent urinary tract infections with renal parenchymal injury, and parental preference. Anti-reflux surgery may be necessary in children with persistent reflux, renal scarring or recurrent pyelonephritis after optimization of bladder and bowel habits. Open, laparoscopic/robot-assisted and endoscopic approaches are all successful in correcting reflux and have been shown to reduce the incidence of febrile urinary tract infections.
Keywords: Pediatrics; Ureteral Diseases; Vesico-Ureteral Reflux.
Copyright® by the International Brazilian Journal of Urology.
Conflict of interest statement
None declared.
Figures
References
-
- Skoog SJ, Peters CA, Arant BS, Jr, Copp HL, Elder JS, Hudson RG, et al. Pediatric Vesicoureteral Reflux Guidelines Panel Summary Report: Clinical Practice Guidelines for Screening Siblings of Children With Vesicoureteral Reflux and Neonates/Infants With Prenatal Hydronephrosis. J Urol. 2010;184:1145–1151. Erratum in: J Urol. 2011;185:365. - PubMed
- 2. Skoog SJ, Peters CA, Arant BS Jr, Copp HL, Elder JS, Hudson RG, et al. Pediatric Vesicoureteral Reflux Guidelines Panel Summary Report: Clinical Practice Guidelines for Screening Siblings of Children With Vesicoureteral Reflux and Neonates/Infants With Prenatal Hydronephrosis. J Urol. 2010;184:1145-51. Erratum in: J Urol. 2011;185:365. - PubMed
-
- Nguyen HT, Herndon CD, Cooper C, Gatti J, Kirsch A, Kokorowski P, et al. The Society for Fetal Urology consensus statement on the evaluation and management of antenatal hydronephrosis. J Pediatr Urol. 2010;6:212–231. - PubMed
- 3. Nguyen HT, Herndon CD, Cooper C, Gatti J, Kirsch A, Kokorowski P, et al. The Society for Fetal Urology consensus statement on the evaluation and management of antenatal hydronephrosis. J Pediatr Urol. 2010;6:212-31. - PubMed
-
- Pokrajac D, Sefic-Pasic I, Begic A. Vesicoureteral Reflux and Renal Scarring in Infants After the First Febrile Urinary Tract Infection. Med Arch. 2018;72:272–275. - PMC - PubMed
- 4. Pokrajac D, Sefic-Pasic I, Begic A. Vesicoureteral Reflux and Renal Scarring in Infants After the First Febrile Urinary Tract Infection. Med Arch. 2018;72:272-5. - PMC - PubMed
-
- Subcommittee on Urinary Tract Infection. Steering Committee on Quality Improvement and Management. Roberts KB. Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics. 2011;128:595–610. - PubMed
- 5. Subcommittee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management, Roberts KB. Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics. 2011;128:595-610. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources