

Modified wallace anastomotic technique reduces ureteroenteric stricture rates after ileal conduit urinary diversion
- PMID: 32167712
- PMCID: PMC7088478
- DOI: 10.1590/S1677-5538.IBJU.2019.0417
Modified wallace anastomotic technique reduces ureteroenteric stricture rates after ileal conduit urinary diversion
Abstract
Purpose: To compare perioperative outcomes, complications and anastomotic stricture rate in a contemporary series of patients who underwent open radical cystectomy (RC) with modified Wallace anastomotic technique versus traditional ileal conduit.
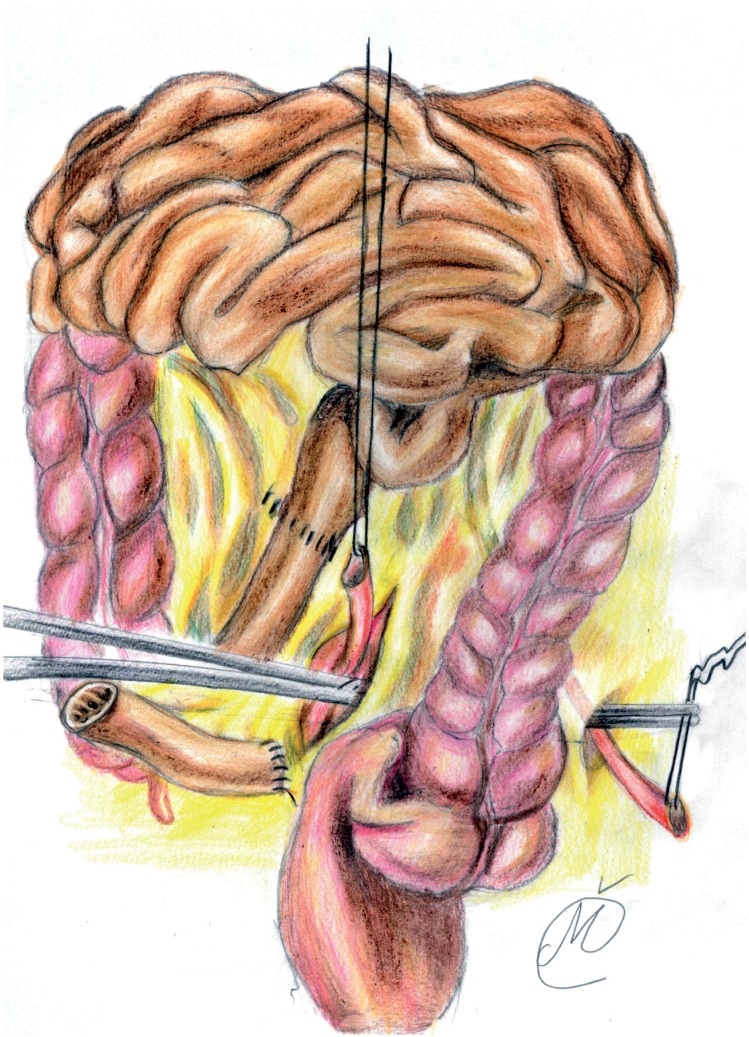
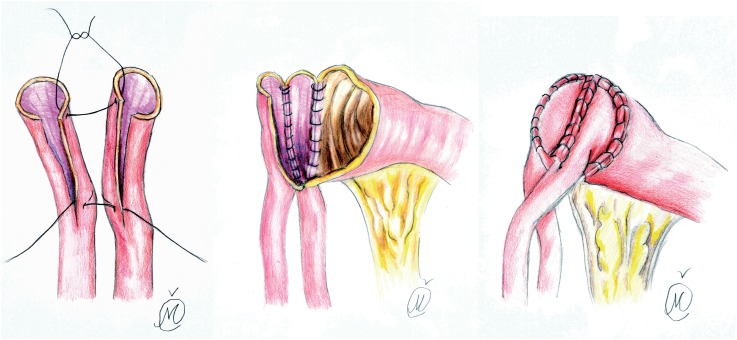
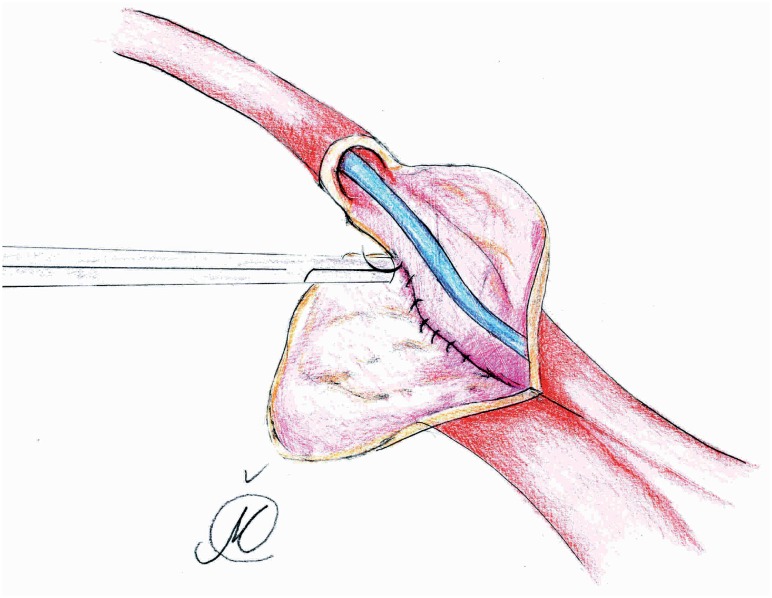
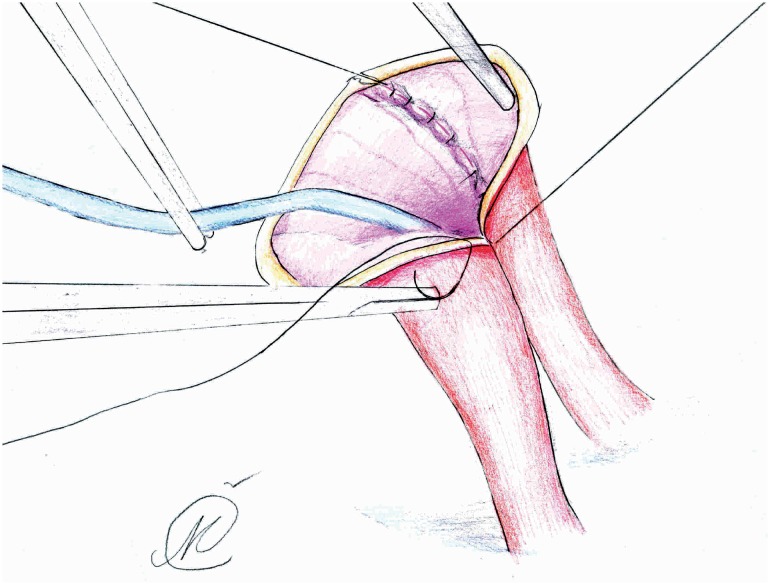
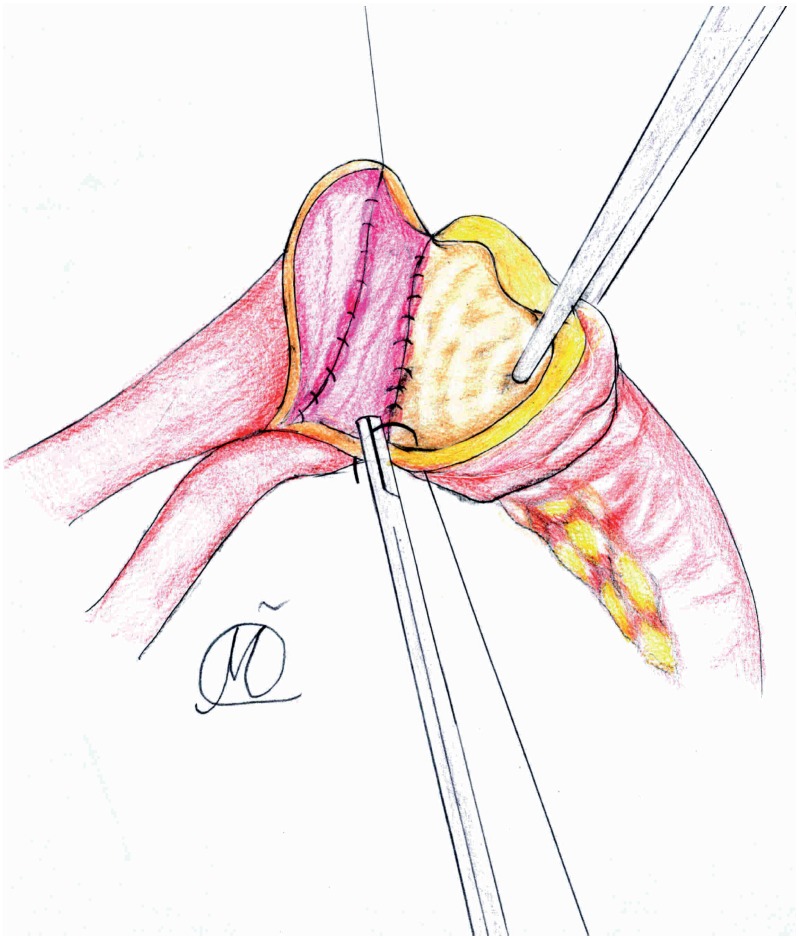
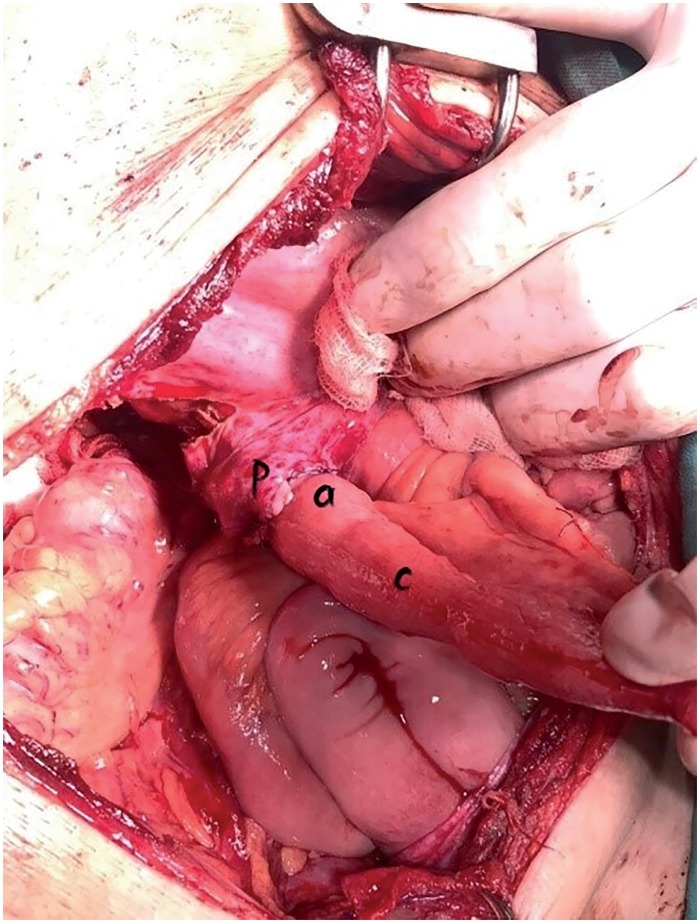
Materials and methods: Study enrolled 180 patients, of whom 140 were randomized and underwent RC; seventy were randomized to group I and the seventy to the group II. For the primary objective, we hypothesized that the rate of ureteroenteric strictures would be at least 20 % lower in the second group. Secondary end points included rate of anastomotic leak, surgical time, deterioration of the upper tract, intraoperative blood loss and patient-reported quality of life (HRQOL). The modified Wallace 1 technique involved eversion of the ureteral plate and bowel mucosa edges, which were anastomosed together in running fashion, while the outher anastomotic wall was augmented with sero-serosal interrupted sutures.
Results: The mean (SD) follow-up time was 26.1 (5.7) months in group I and 25.2 (4.8) months in group II, during which, anastomotic stricture was observed in 8 patients (12%) from the first and 2 patients (3%) from the second group (p < 0.05). The anastomotic leakage rate was significantly higher in first group (17% vs. 8.5%, p < 0.05), while patient-reported HRQOL outcomes were similar between groups after the 12 month follow-up period.
Conclusions: By using a modified Wallace technique, we were able to significantly lower anastomotic stricture and anastomotic leakage rates, which are major issues in minimizing both short- and long-term postoperative complications.
Keywords: Cystectomy; Quality of Life; Urinary Diversion.
Copyright® by the International Brazilian Journal of Urology.
Conflict of interest statement
None declared.
Figures
References
-
- Davis NF, Burke JP, McDermott T, Flynn R, Manecksha RP, Thornhill JA. Bricker versus Wallace anastomosis: A metaanalysis of ureteroenteric stricture rates after ileal conduit urinary diversion. Can Urol Assoc J. 2015;9:E284–E290. - PMC - PubMed
- 1. Davis NF, Burke JP, McDermott T, Flynn R, Manecksha RP, Thornhill JA. Bricker versus Wallace anastomosis: A metaanalysis of ureteroenteric stricture rates after ileal conduit urinary diversion. Can Urol Assoc J. 2015;9:E284-90. - PMC - PubMed
-
- Evangelidis A, Lee EK, Karellas ME, Thrasher JB, Holzbeierlein JM. Evaluation of ureterointestinal anastomosis: Wallace vs Bricker. J Urol. 2006;175:1755–1758. - PubMed
- 2. Evangelidis A, Lee EK, Karellas ME, Thrasher JB, Holzbeierlein JM. Evaluation of ureterointestinal anastomosis: Wallace vs Bricker. J Urol. 2006;175:1755-8. - PubMed
-
- Ficarra V, Giannarini G, Crestani A, Palumbo V, Rossanese M, Valotto C, et al. Retrosigmoid Versus Traditional Ileal Conduit for Urinary Diversion After Radical Cystectomy. Eur Urol. 2019;75:294–299. - PubMed
- 3. Ficarra V, Giannarini G, Crestani A, Palumbo V, Rossanese M, Valotto C, et al. Retrosigmoid Versus Traditional Ileal Conduit for Urinary Diversion After Radical Cystectomy. Eur Urol. 2019;75:294-9. - PubMed
-
- Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85:365–376. - PubMed
- 4. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85:365-76. - PubMed
-
- Singh V, Yadav R, Sinha RJ, Gupta DK. Prospective comparison of quality-of-life outcomes between ileal conduit urinary diversion and orthotopic neobladder reconstruction after radical cystectomy: a statistical model. BJU Int. 2014;113:726–732. - PubMed
- 5. Singh V, Yadav R, Sinha RJ, Gupta DK. Prospective comparison of quality-of-life outcomes between ileal conduit urinary diversion and orthotopic neobladder reconstruction after radical cystectomy: a statistical model. BJU Int. 2014;113:726-32. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical