

Physical Rehabilitation in Critically Ill Children: A Multicenter Point Prevalence Study in the United States
- PMID: 32168030
- PMCID: PMC7539558
- DOI: 10.1097/CCM.0000000000004291
Physical Rehabilitation in Critically Ill Children: A Multicenter Point Prevalence Study in the United States
Abstract
Objectives: With decreasing mortality in PICUs, a growing number of survivors experience long-lasting physical impairments. Early physical rehabilitation and mobilization during critical illness are safe and feasible, but little is known about the prevalence in PICUs. We aimed to evaluate the prevalence of rehabilitation for critically ill children and associated barriers.
Design: National 2-day point prevalence study.
Setting: Eighty-two PICUs in 65 hospitals across the United States.
Patients: All patients admitted to a participating PICU for greater than or equal to 72 hours on each point prevalence day.
Interventions: None.
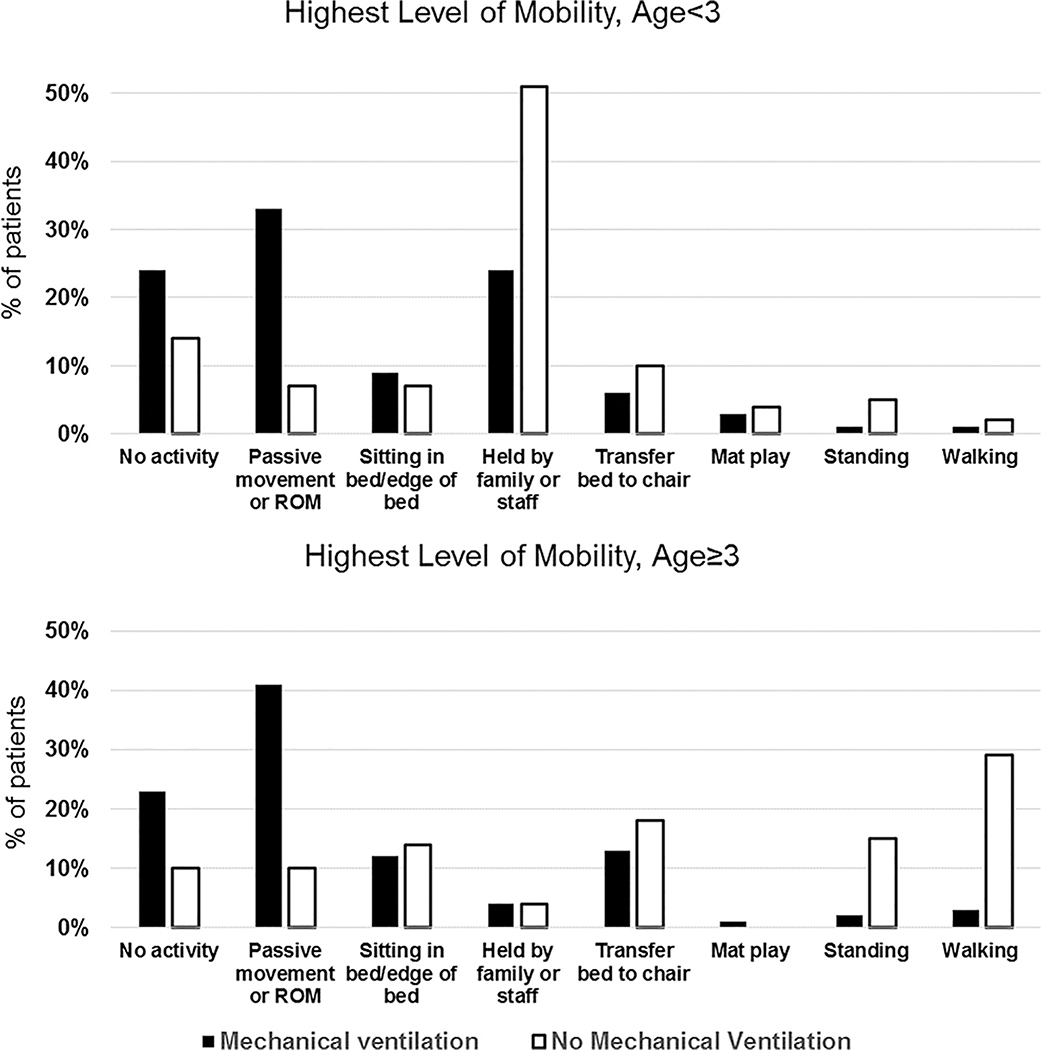
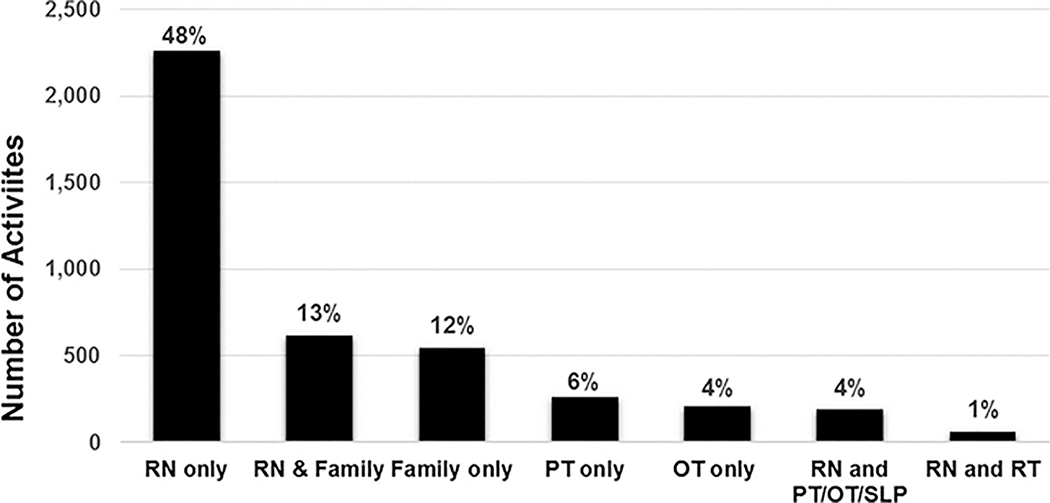
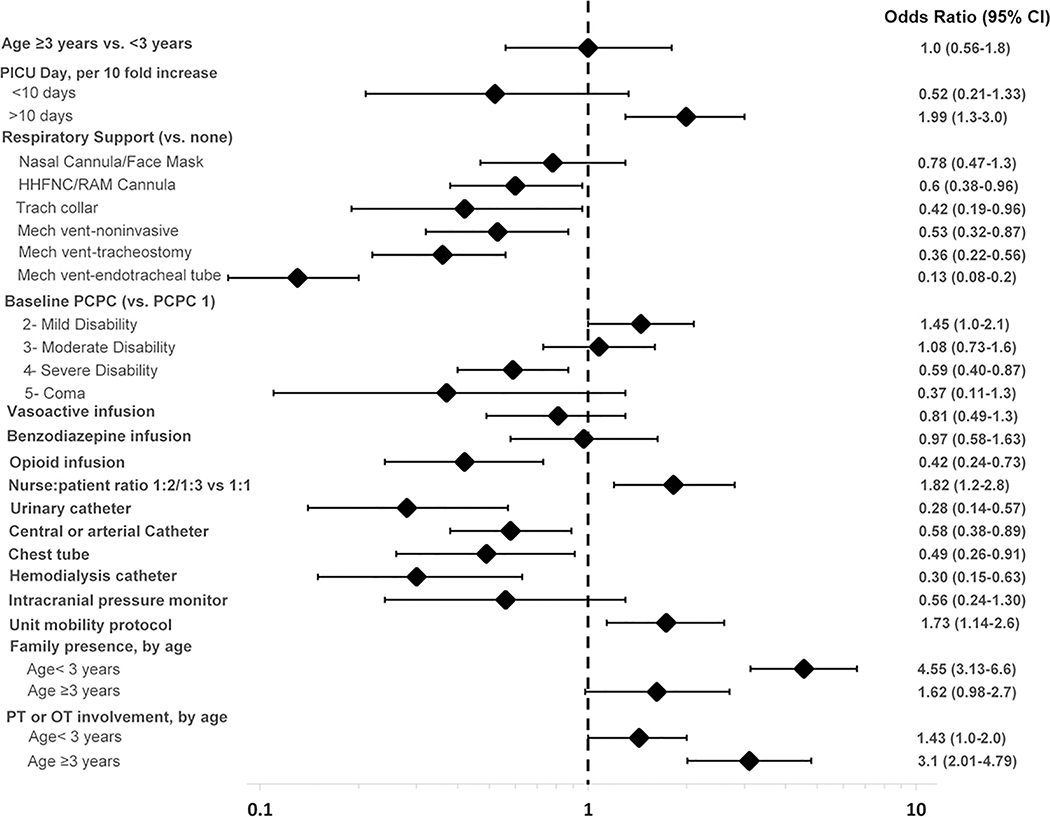
Measurements and main results: The primary outcome was prevalence of physical therapy- or occupational therapy-provided mobility on the study days. PICUs also prospectively collected timing of initial rehabilitation team consultation, clinical and patient mobility data, potential mobility-associated safety events, and barriers to mobility. The point prevalence of physical therapy- or occupational therapy-provided mobility during 1,769 patient-days was 35% and associated with older age (adjusted odds ratio for 13-17 vs < 3 yr, 2.1; 95% CI, 1.5-3.1) and male gender (adjusted odds ratio for females, 0.76; 95% CI, 0.61-0.95). Patients with higher baseline function (Pediatric Cerebral Performance Category, ≤ 2 vs > 2) less often had rehabilitation consultation within the first 72 hours (27% vs 38%; p < 0.001). Patients were completely immobile on 19% of patient-days. A potential safety event occurred in only 4% of 4,700 mobility sessions, most commonly a transient change in vital signs. Out-of-bed mobility was negatively associated with the presence of an endotracheal tube (adjusted odds ratio, 0.13; 95% CI, 0.1-0.2) and urinary catheter (adjusted odds ratio, 0.28; 95% CI, 0.1-0.6). Positive associations included family presence in children less than 3 years old (adjusted odds ratio, 4.55; 95% CI, 3.1-6.6).
Conclusions: Younger children, females, and patients with higher baseline function less commonly receive rehabilitation in U.S. PICUs, and early rehabilitation consultation is infrequent. These findings highlight the need for systematic design of rehabilitation interventions for all critically ill children at risk of functional impairments.
Conflict of interest statement
Figures
References
-
- Devlin JW, Skrobik Y, Gelinas C, et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit Care Med 2018;46(9):e825–e873. - PubMed
-
- Cummins KA, Watters R, Leming-Lee T. Reducing Pressure Injuries in the Pediatric Intensive Care Unit. Nurs Clin North Am 2019;54(1):127–140. - PubMed
-
- Curley MA, Quigley SM, Lin M. Pressure ulcers in pediatric intensive care: incidence and associated factors. Pediatr Crit Care Med 2003;4(3):284–290. - PubMed
