

Deep Convolutional Neural Network-Based Diagnosis of Anterior Cruciate Ligament Tears: Performance Comparison of Homogenous Versus Heterogeneous Knee MRI Cohorts With Different Pulse Sequence Protocols and 1.5-T and 3-T Magnetic Field Strengths
- PMID: 32168039
- PMCID: PMC7343178
- DOI: 10.1097/RLI.0000000000000664
Deep Convolutional Neural Network-Based Diagnosis of Anterior Cruciate Ligament Tears: Performance Comparison of Homogenous Versus Heterogeneous Knee MRI Cohorts With Different Pulse Sequence Protocols and 1.5-T and 3-T Magnetic Field Strengths
Abstract
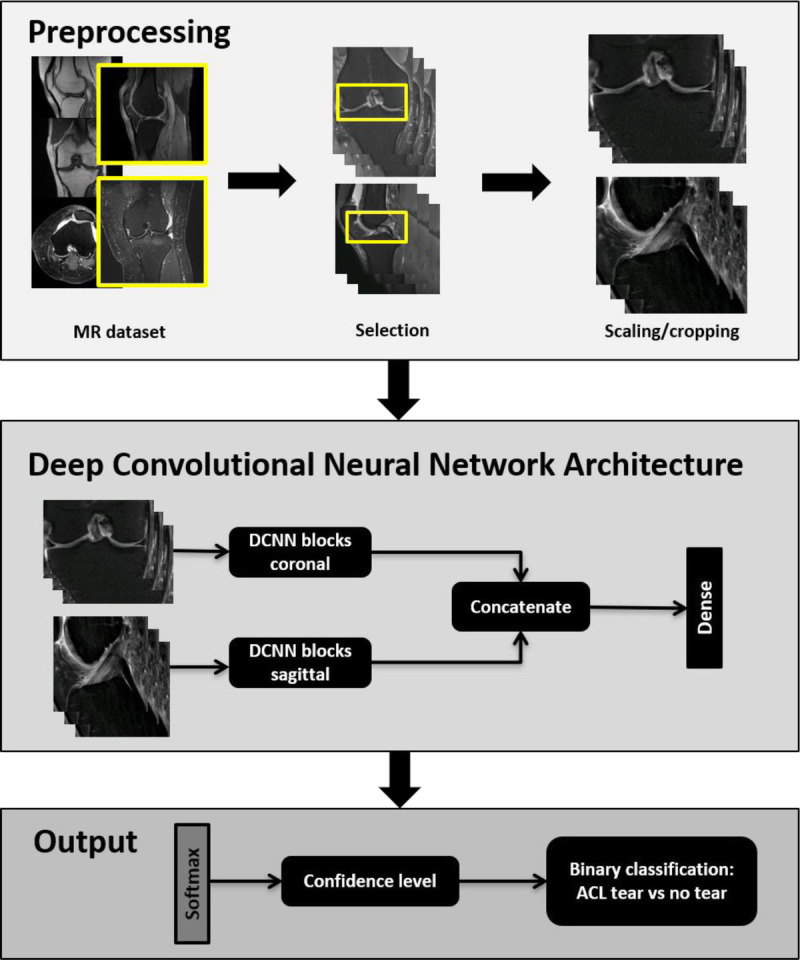
Objectives: The aim of this study was to clinically validate a Deep Convolutional Neural Network (DCNN) for the detection of surgically proven anterior cruciate ligament (ACL) tears in a large patient cohort and to analyze the effect of magnetic resonance examinations from different institutions, varying protocols, and field strengths.
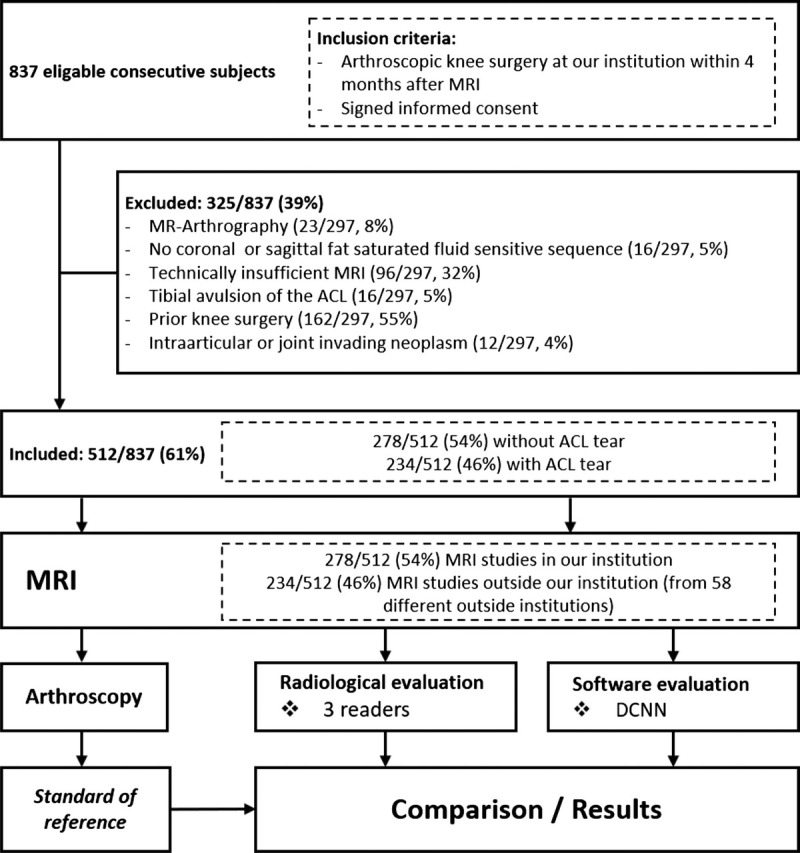
Materials and methods: After ethics committee approval, this retrospective analysis of prospectively collected data was performed on 512 consecutive subjects, who underwent knee magnetic resonance imaging (MRI) in a total of 59 different institutions followed by arthroscopic knee surgery at our institution. The DCNN and 3 fellowship-trained full-time academic musculoskeletal radiologists evaluated the MRI examinations for full-thickness ACL tears independently. Surgical reports served as the reference standard. Statistics included diagnostic performance metrics, including sensitivity, specificity, area under the receiver operating curve ("AUC ROC"), and kappa statistics. P values less than 0.05 were considered to represent statistical significance.
Results: Anterior cruciate ligament tears were present in 45.7% (234/512) and absent in 54.3% (278/512) of the subjects. The DCNN had a sensitivity of 96.1%, which was not significantly different from the readers (97.5%-97.9%; all P ≥ 0.118), but significantly lower specificity of 93.1% (readers, 99.6%-100%; all P < 0.001) and "AUC ROC" of 0.935 (readers, 0.989-0.991; all P < 0.001) for the entire cohort. Subgroup analysis showed a significantly lower sensitivity, specificity, and "AUC ROC" of the DCNN for outside MRI (92.5%, 87.1%, and 0.898, respectively) than in-house MRI (99.0%, 94.4%, and 0.967, respectively) examinations (P = 0.026, P = 0.043, and P < 0.05, respectively). There were no significant differences in DCNN performance for 1.5-T and 3-T MRI examinations (all P ≥ 0.753, respectively).
Conclusions: Deep Convolutional Neural Network performance of ACL tear diagnosis can approach performance levels similar to fellowship-trained full-time academic musculoskeletal radiologists at 1.5 T and 3 T; however, the performance may decrease with increasing MRI examination heterogeneity.
Conflict of interest statement
Conflicts of interest and sources of funding: Giuseppe Marbach and Francesco Civardi are employees of Balzano Informatik AG. Jan Fritz received institutional research support from Siemens Healthcare USA, DePuy, Zimmer, Microsoft, and BTG International; is a scientific advisor for Siemens Healthcare USA, GE Healthcare Technologies, and BTG International; and has shared patents with Siemens Healthcare and Johns Hopkins University. The other authors report no conflicts of interest.
Figures
References
-
- Salzler M, Nwachukwu BU, Rosas S, et al. State-of-the-art anterior cruciate ligament tears: a primer for primary care physicians. Phys Sportsmed. 2015;43:169–177. - PubMed
-
- Morelli V, Bright C, Fields A. Ligamentous injuries of the knee: anterior cruciate, medial collateral, posterior cruciate, and posterolateral corner injuries. Prim Care. 2013;40:335–356. - PubMed
-
- Hewett TE, Myer GD, Ford KR. Anterior cruciate ligament injuries in female athletes: part 1, mechanisms and risk factors. Am J Sports Med. 2006;34:299–311. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
