

Characterization of the immune cell landscape of patients with NAFLD
- PMID: 32168345
- PMCID: PMC7069622
- DOI: 10.1371/journal.pone.0230307
Characterization of the immune cell landscape of patients with NAFLD
Abstract
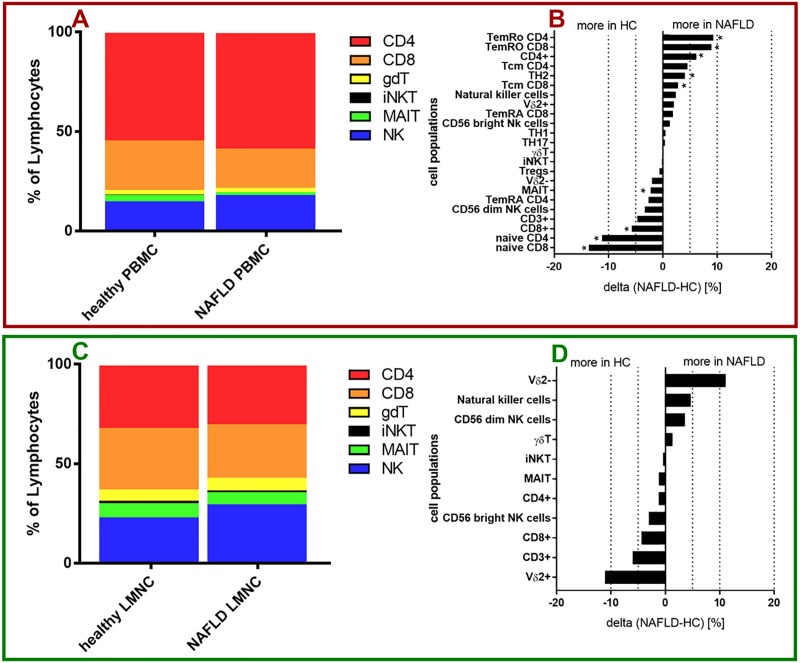
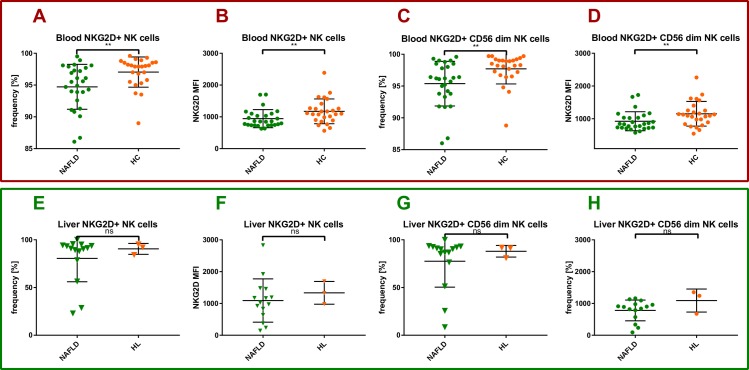
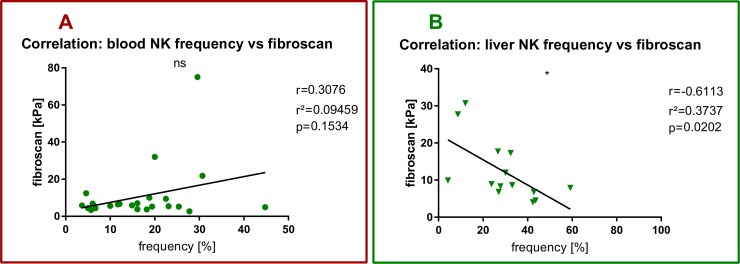
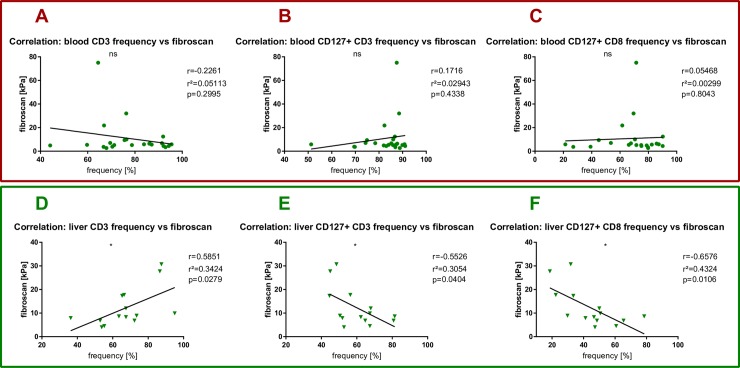
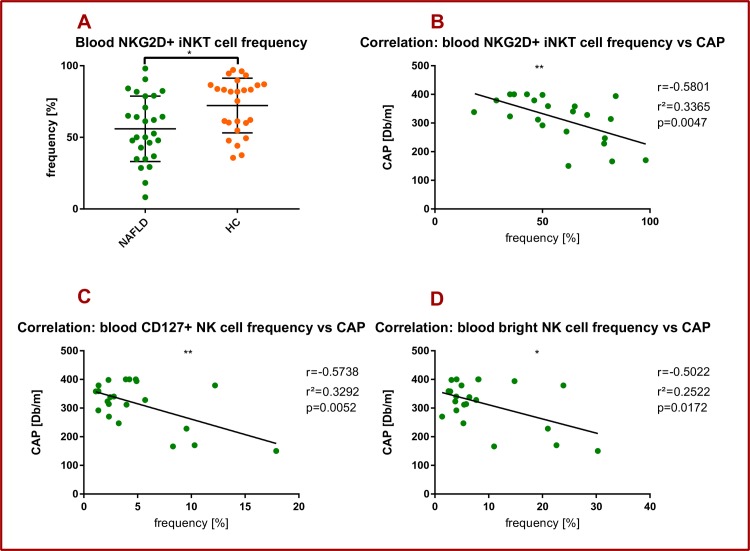
Multiple factors are involved in the pathogenesis of non-alcoholic fatty liver disease (NAFLD), but the exact immunological mechanisms that cause inflammation and fibrosis of the liver remain enigmatic. In this current study, cellular samples of a cohort of NAFLD patients (peripheral blood mononuclear cells (PBMC): n = 27, liver samples: n = 15) and healthy individuals (PBMC: n = 26, liver samples: n = 3) were analyzed using 16-color flow cytometry, and the frequency and phenotype of 23 immune cell subtypes was assessed. PBMC of NAFLD patients showed decreased frequencies of total CD3+, CD8+ T cells, CD56dim NK cells and MAIT cells, but elevated frequencies of CD4+ T cells and Th2 cells compared to healthy controls. Intrahepatic lymphocytes (IHL) of NAFLD patients showed decreased frequencies of total T cells, total CD8+ T cells, Vd2+γδ T cells, and CD56bright NK cells, but elevated frequencies of Vδ2-γδ T cells and CD56dim NK cells compared to healthy controls. The activating receptor NKG2D was significantly less frequently expressed among iNKT cells, total NK cells and CD56dim NK cells of PBMC of NAFLD patients compared to healthy controls. More strikingly, hepatic fibrosis as measured by fibroscan elastography negatively correlated with the intrahepatic frequency of total NK cells (r2 = 0,3737, p = 0,02). Hepatic steatosis as measured by controlled attenuation parameter (CAP) value negatively correlated with the frequency of circulating NKG2D+ iNKT cells (r2 = 0,3365, p = 0,0047). Our data provide an overview of the circulating and intrahepatic immune cell composition of NAFLD patients, and point towards a potential role of NK cells and iNKT cells for the regulation of hepatic fibrosis and steatosis in NAFLD.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
