

Neurological and psychiatric safety of tafenoquine in Plasmodium vivax relapse prevention: a review
- PMID: 32169086
- PMCID: PMC7071640
- DOI: 10.1186/s12936-020-03184-x
Neurological and psychiatric safety of tafenoquine in Plasmodium vivax relapse prevention: a review
Abstract
Background: Tafenoquine is an 8-aminoquinoline anti-malarial drug recently approved as a single-dose (300 mg) therapy for Plasmodium vivax relapse prevention, when co-administered with 3-days of chloroquine or other blood schizonticide. Tafenoquine 200 mg weekly after a loading dose is also approved as travellers' prophylaxis. The development of tafenoquine has been conducted over many years, using various dosing regimens in diverse populations.
Methods: This review brings together all the preclinical and clinical data concerning tafenoquine central nervous system safety. Data were assembled from published sources. The risk of neuropsychiatric adverse events (NPAEs) with single-dose tafenoquine (300 mg) in combination with chloroquine to achieve P. vivax relapse prevention is particularly examined.
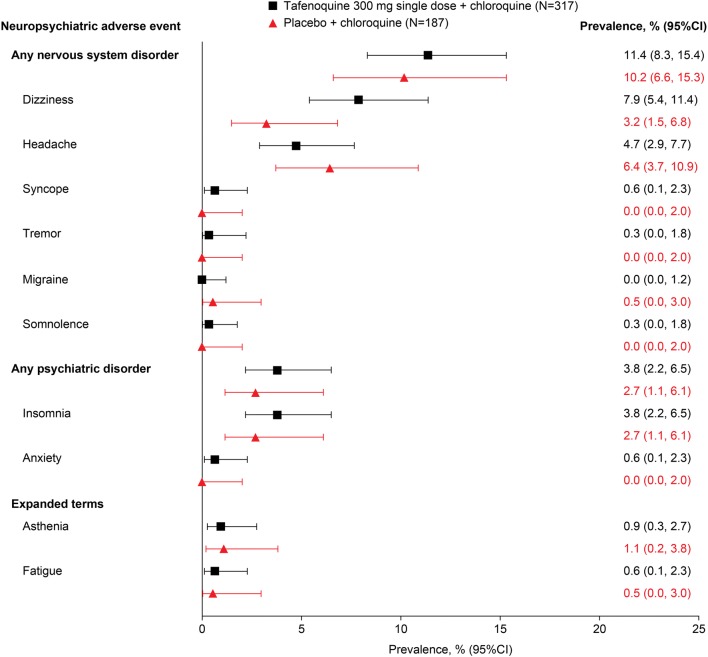
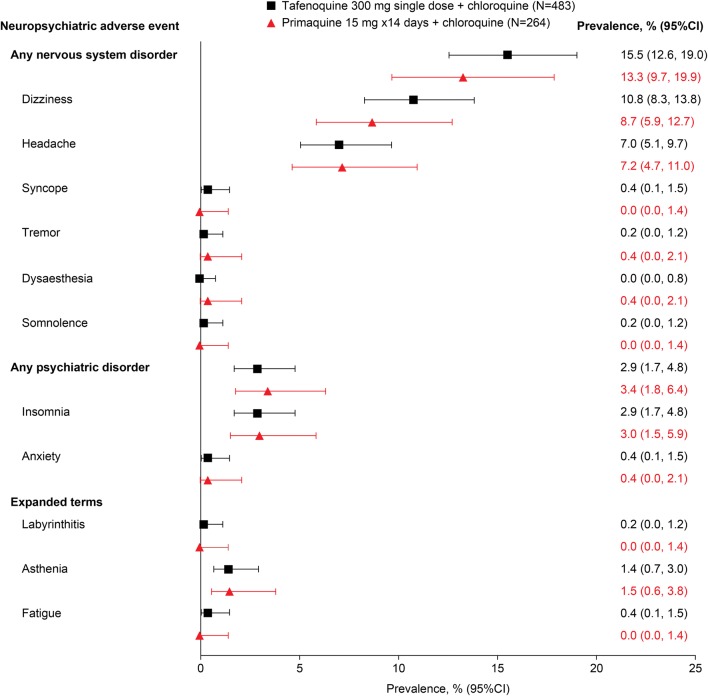
Results: There was no evidence of neurotoxicity with tafenoquine in preclinical animal models. In clinical studies in P. vivax relapse prevention, nervous system adverse events, mainly headache and dizziness, occurred in 11.4% (36/317) of patients with tafenoquine (300 mg)/chloroquine versus 10.2% (19/187) with placebo/chloroquine; and in 15.5% (75/483) of patients with tafenoquine/chloroquine versus 13.3% (35/264) with primaquine (15 mg/day for 14 days)/chloroquine. Psychiatric adverse events, mainly insomnia, occurred in 3.8% (12/317) of patients with tafenoquine/chloroquine versus 2.7% (5/187) with placebo/chloroquine; and in 2.9% (14/483) of patients with tafenoquine/chloroquine versus 3.4% (9/264) for primaquine/chloroquine. There were no serious or severe NPAEs observed with tafenoquine (300 mg)/chloroquine in these studies.
Conclusions: The risk:benefit of single-dose tafenoquine/chloroquine in P. vivax relapse prevention is favourable in the presence of malaria, with a low risk of NPAEs, similar to that seen with chloroquine alone or primaquine/chloroquine.
Keywords: Adverse events; Anti-malarial; Malaria; Neuropsychiatric; Tafenoquine.
Conflict of interest statement
Stephan Duparc and Stephan Chalon are employees of Medicines for Malaria Venture. Scott Miller is an employee of the Bill and Melinda Gates Foundation. Scott Miller is a retired U. S. Army officer, and his views are his own and not those of the U.S. Army or the U.S. Department of Defense. Naomi Richardson received funding from Medicines for Malaria Venture in regard to this article and has been previously employed as an external communications consultant by GlaxoSmithKline and Medicines for Malaria Venture. Stephen Toovey has been employed as a consultant to Medicines for Malaria Venture in regard to this article and to GlaxoSmithKline and 60P Pharmaceuticals.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
