

Molecular and immunological features of a prolonged exceptional responder with malignant pleural mesothelioma treated initially and rechallenged with pembrolizumab
- PMID: 32169873
- PMCID: PMC7069263
- DOI: 10.1136/jitc-2020-000713
Molecular and immunological features of a prolonged exceptional responder with malignant pleural mesothelioma treated initially and rechallenged with pembrolizumab
Abstract
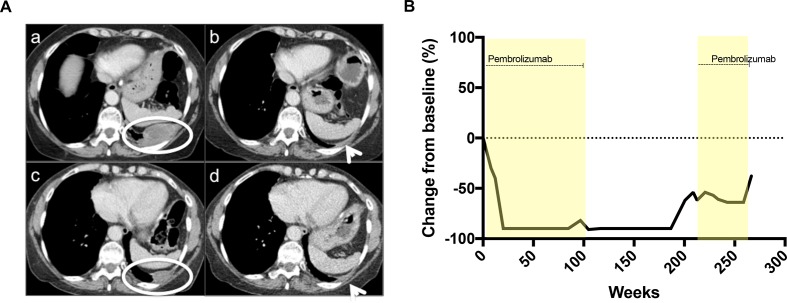
Background: This case represents an exceptional response to pembrolizumab in a patient with epithelioid mesothelioma with a further response on rechallenge.
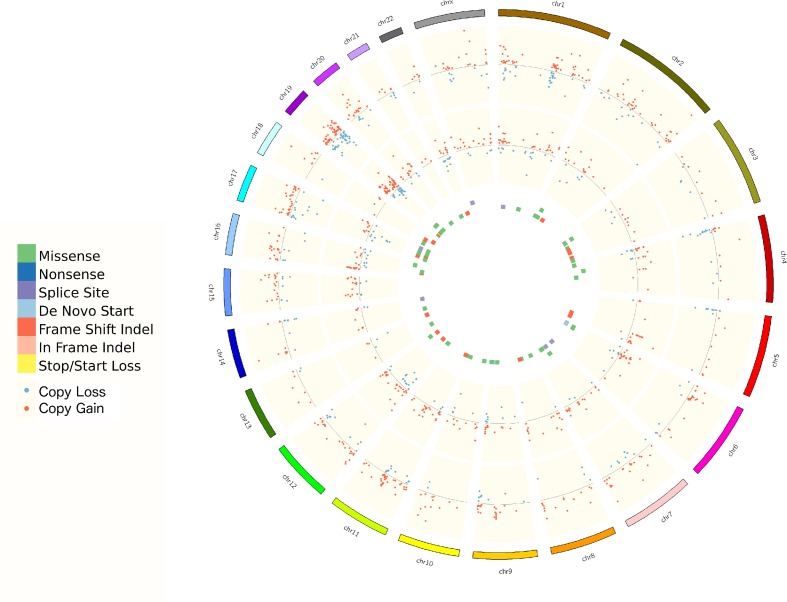
Case presentation: A 77-year-old woman with advanced epithelioid mesothelioma extensively pretreated with chemotherapy demonstrated a prolonged response of 45 months to 52 cycles of pembrolizumab. On rechallenge with pembrolizumab, further disease stability was achieved. Serial biopsies and analysis by immunohistochemistry and immunofluorescence demonstrated marked immune infiltration and documented the emergency of markers of immune exhaustion. Whole exome sequencing demonstrated a reduction in tumor mutational burden consistent with subclone elimination by immune checkpoint inhibitor (CPI) therapy. The relapse biopsy had missense mutation in BTN2A1.
Conclusion: This case supports rechallenge of programme death receptor 1 inhibitor in cases of previous CPI sensitivity and gives molecular insights.
Keywords: PD-1; PD-L1; TMB; immunotherapy; mesothelioma.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: AM: honoraria from FARON and Bayer. AW: advisory boards for Bayer, Bristol-Myers Sqibb and Celgene. SP: honoraria from Boehringer Ingelheim, AstraZeneca, Roche, Takeda and Chugai Pharma; advisory boards from Boehringer Ingelheim, AstraZeneca, Roche, Novartis, Pfizer, Bristol-Myer Squibb, MSD, Guardant Health, Abbvie, EMD Serono and Takeda; expenses from Boehringer Ingelheim, Bristol-Myer Squibb and Merck Sharp & Dohme. MO: advisory boards for MSD, Abbvie, BMS, BI, Pierre Fabre. UB: honoraria from Astellas, Novartis, Karus Therapeutics, Phoenix Solutions, Eli Lilly, Astex and Vernalis; funding for phase I investigator-initiated trials from Onyx Pharmaceuticals, BTG International, Chugai, Astrazeneca and Verastem. JdB: personal fees and non-financial support from Astellas Pharma, Genentech/Roche, Pfizer, Sanofi, Bayer, Boehringer Ingelheim, Merck Serono and Merck Sharp & Dohme; grants, personal fees and non-financial support from AstraZeneca; non-financial support from Genmab, GlaxoSmithKline, Orion Pharma GmbH, Qiagen, Taiho Pharmaceutical and Vertex. In addition, JdB has a patent Abiraterone Rewards to Inventors with royalties paid to institution, no personal income and a patent PARP inhibitors and DNA repair defects with royalties paid to institution, no personal income. JL: research funding from Roche Genentech, Genmab and Basilea Travel from Basilea.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials