

Analysing The Cross-Section of The Abdominal Aortic Aneurysm Neck and Its Effects on Stent Deployment
- PMID: 32170088
- PMCID: PMC7070033
- DOI: 10.1038/s41598-020-61578-y
Analysing The Cross-Section of The Abdominal Aortic Aneurysm Neck and Its Effects on Stent Deployment
Abstract
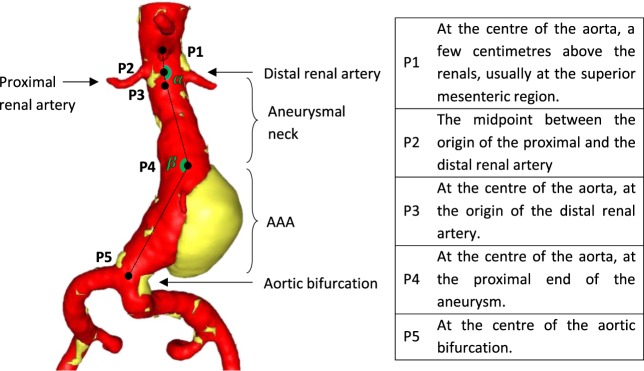
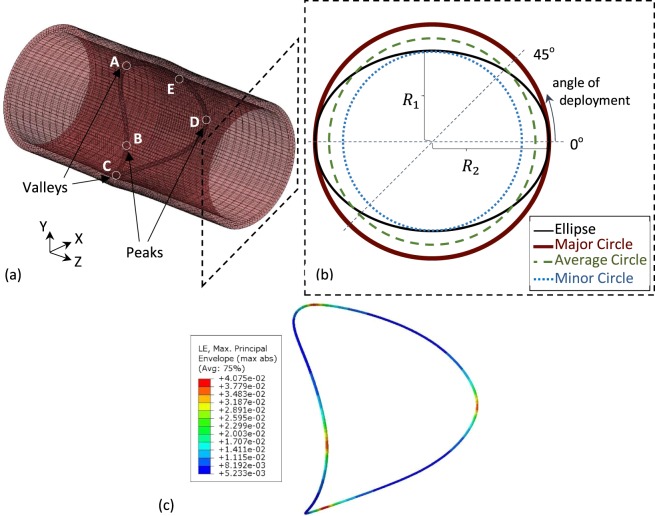
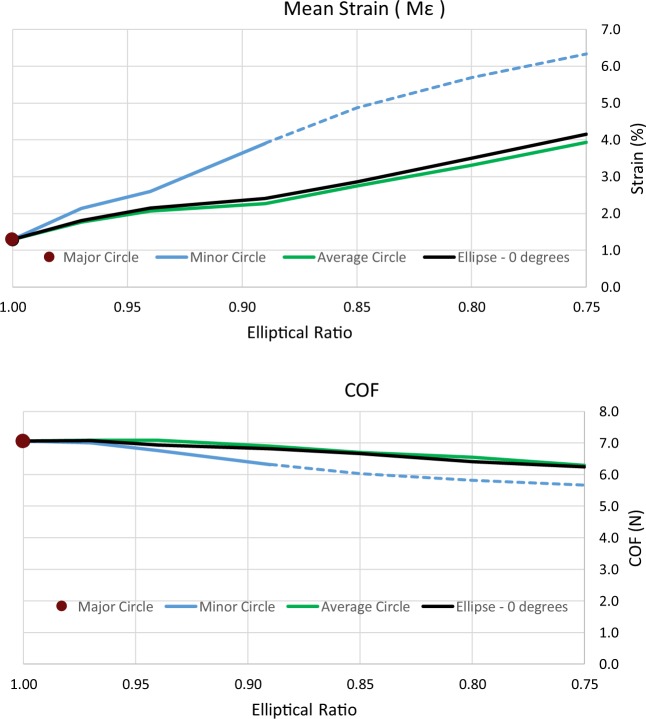
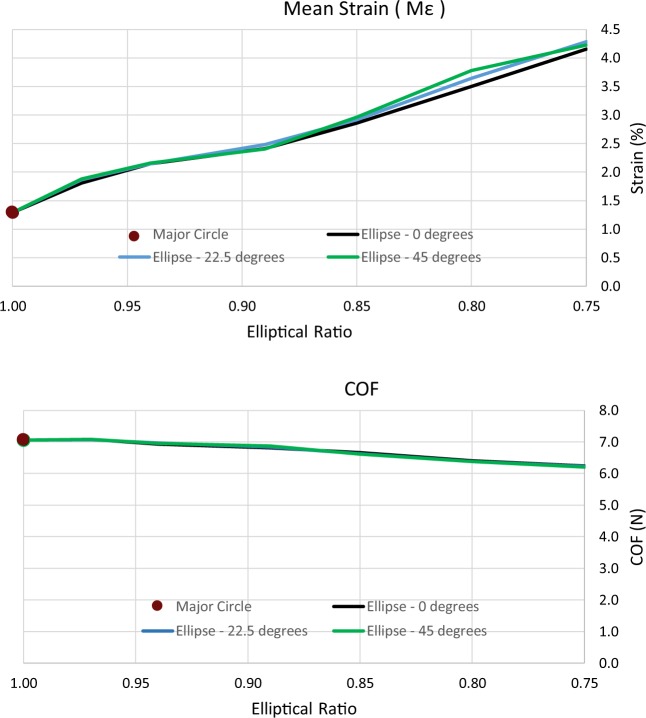
Stent graft devices for the treatment of abdominal aortic aneurysms (AAAs) are being increasingly used worldwide. Yet, during modelling and optimization of these devices, as well as in clinical practice, vascular sections are idealized, possibly compromising the effectiveness of the intervention. In this study, we challenge the commonly used approximation of the circular cross-section of the aorta and identify the implications of this approximation to the mechanical assessment of stent grafts. Using computed tomography angiography (CTA) data from 258 AAA patients, the lumen of the aneurysmal neck was analysed. The cross-section of the aortic neck was found to be an independent variable, uncorrelated to other geometrical aspects of the region, and its shape was non-circular reaching elliptical ratios as low as 0.77. These results were used to design a finite element analysis (FEA) study for the assessment of a ring stent bundle deployed under a variety of aortic cross-sections. Results showed that the most common clinical approximations of the vascular cross-section can be a source of significant error when calculating the maximum stent strains (underestimated by up to 69%) and radial forces (overestimated by up to 13%). Nevertheless, a less frequently used average approximation was shown to yield satisfactory results (5% and 2% of divergence respectively).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Predisposing Factors for Migration of the Iliac Limb and Reintervention after Endovascular Abdominal Aortic Aneurysm Repair.Ann Vasc Surg. 2019 Aug;59:91-101. doi: 10.1016/j.avsg.2019.01.007. Epub 2019 Apr 19. Ann Vasc Surg. 2019. PMID: 31009727
-
Clinical Outcomes of Endovascular Aneurysm Repair with the Kilt Technique for Abdominal Aortic Aneurysms with Hostile Aneurysm Neck Anatomy: A Korean Multicenter Retrospective Study.Cardiovasc Intervent Radiol. 2018 Apr;41(4):554-563. doi: 10.1007/s00270-017-1867-y. Epub 2017 Dec 26. Cardiovasc Intervent Radiol. 2018. PMID: 29279976
-
The Relationship between Temporal Changes in Proximal Neck Angulation and Stent-Graft Migration after Endovascular Abdominal Aortic Aneurysm Repair.Ann Vasc Surg. 2017 Feb;39:119-127. doi: 10.1016/j.avsg.2016.05.128. Epub 2016 Aug 24. Ann Vasc Surg. 2017. PMID: 27565407
-
Endovascular repair of abdominal aortic aneurysm with severely angulated neck and tortuous artery access: case report and literature review.BMC Surg. 2015 Mar 8;15:20. doi: 10.1186/s12893-015-0005-5. BMC Surg. 2015. PMID: 25887163 Free PMC article. Review.
-
Use of Endurant Stent-Graft Aortic Extensions for the Treatment of Focal Aortic Pathology.Ann Vasc Surg. 2016 Oct;36:99-105. doi: 10.1016/j.avsg.2016.03.017. Epub 2016 Jul 13. Ann Vasc Surg. 2016. PMID: 27421197 Review.
Cited by
-
Buckling of Arteries With Noncircular Cross Sections: Theory and Finite Element Simulations.Front Physiol. 2021 Aug 13;12:712636. doi: 10.3389/fphys.2021.712636. eCollection 2021. Front Physiol. 2021. PMID: 34483964 Free PMC article.
-
Imaging Predictive Factors of Abdominal Aortic Aneurysm Growth.J Clin Med. 2021 Apr 28;10(9):1917. doi: 10.3390/jcm10091917. J Clin Med. 2021. PMID: 33925046 Free PMC article. Review.
-
PCSK9, a novel immune and ferroptosis related gene in abdominal aortic aneurysm neck.Sci Rep. 2023 Apr 13;13(1):6054. doi: 10.1038/s41598-023-33287-9. Sci Rep. 2023. PMID: 37055467 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
