

Alternative and complementary therapies in osteoarthritis and cartilage repair
- PMID: 32170710
- PMCID: PMC7170824
- DOI: 10.1007/s40520-020-01515-1
Alternative and complementary therapies in osteoarthritis and cartilage repair
Abstract
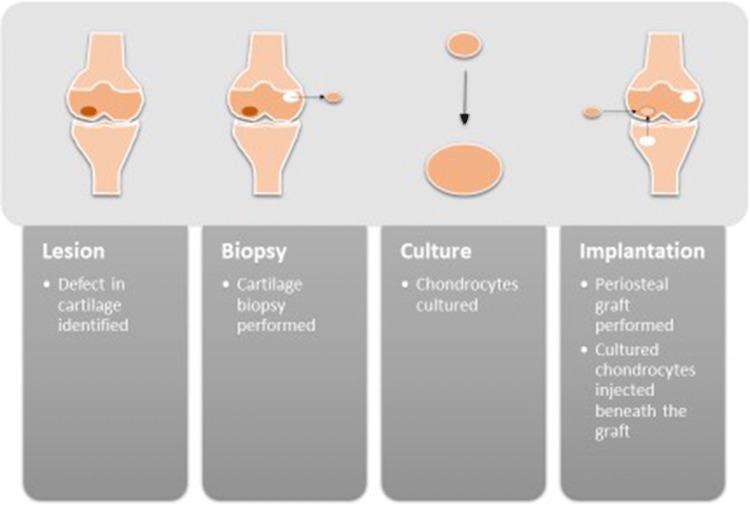
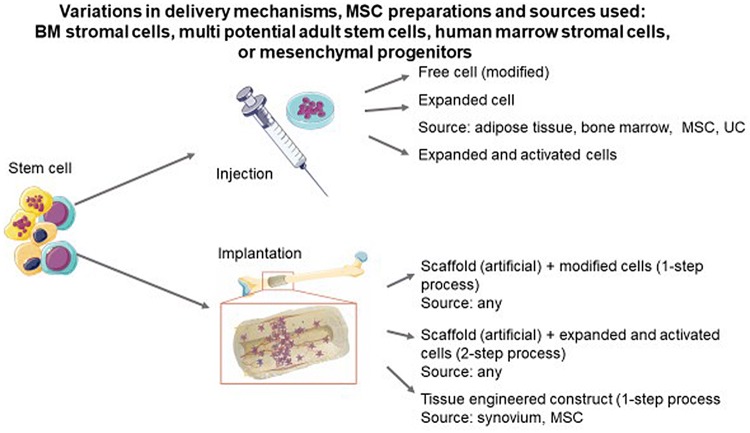
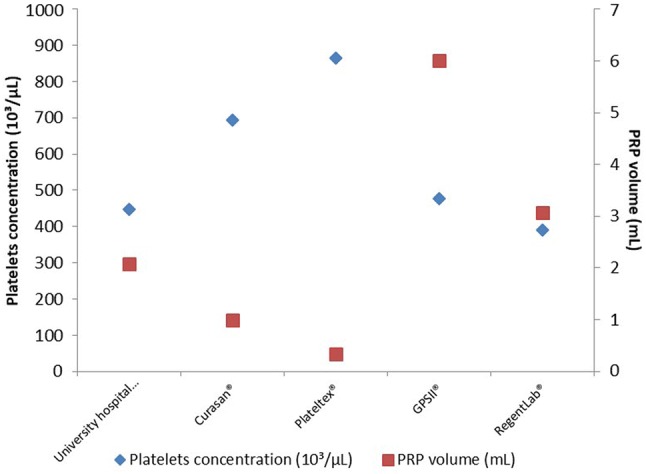
Osteoarthritis (OA) is the most common joint condition and, with a burgeoning ageing population, is due to increase in prevalence. Beyond conventional medical and surgical interventions, there are an increasing number of 'alternative' therapies. These alternative therapies may have a limited evidence base and, for this reason, are often only afforded brief reference (or completely excluded) from current OA guidelines. Thus, the aim of this review was to synthesize the current evidence regarding autologous chondrocyte implantation (ACI), mesenchymal stem cell (MSC) therapy, platelet-rich plasma (PRP), vitamin D and other alternative therapies. The majority of studies were in knee OA or chondral defects. Matrix-assisted ACI has demonstrated exceedingly limited, symptomatic improvements in the treatment of cartilage defects of the knee and is not supported for the treatment of knee OA. There is some evidence to suggest symptomatic improvement with MSC injection in knee OA, with the suggestion of minimal structural improvement demonstrated on MRI and there are positive signals that PRP may also lead to symptomatic improvement, though variation in preparation makes inter-study comparison difficult. There is variability in findings with vitamin D supplementation in OA, and the only recommendation which can be made, at this time, is for replacement when vitamin D is deplete. Other alternative therapies reviewed have some evidence (though from small, poor-quality studies) to support improvement in symptoms and again there is often a wide variation in dosage and regimens. For all these therapeutic modalities, although controlled studies have been undertaken to evaluate effectiveness in OA, these have often been of small size, limited statistical power, uncertain blindness and using various methodologies. These deficiencies must leave the question as to whether they have been validated as effective therapies in OA (or chondral defects). The conclusions of this review are that all alternative interventions definitely require clinical trials with robust methodology, to assess their efficacy and safety in the treatment of OA beyond contextual and placebo effects.
Keywords: Alternative; Cartilage; Herbal; Osteoarthritis; Therapy; Treatment.
Conflict of interest statement
NRF, ROCO, AJP, JFK, MC, GH, JB, NV, AAK, RM, MV, WL, RRo, NA-D and RRi have no relevant conflicts of interest to declare. CC has received lecture fees and honoraria from Amgen, Danone, Eli Lilly, GSK, Kyowa Kirin, Medtronic, Merck, Nestlé, Novartis, Pfizer, Roche, Servier, Shire, Takeda and UCB outside of the submitted work. EM reports personal fees from Expanscience, personal fees from Mylan - Meda, personal fees from TRB Chemedica, Pierre Fabre, Celgène and Fidia, and non-financial support from Pfizer, outside the submitted work. PGC reports personal fees from AbbVie, personal fees from Flexion Therapeutics, personal fees from Galapagos, personal fees from GlaxoSmithKline, personal fees from Novartis, personal fees from Pfizer, personal fees from Samumed, outside the submitted work. FB reports personal fees from 4P Pharma, Boehringer, Bone Therapeutics, Expanscience, Galapagos, Gilead, GSK, Heel, Merck Sereno, MSD, Nordic, Novartis, Peptinov, Pfizer, Regulaxis, Roche, Sandoz, Sanofi, Servier, TRB Chemedica, UCB. MLB reports grants and honoraria from AMGEN, grants from ABIOGEN, grants and consultancy from ALEXION, grants, consultant and honoraria from BRUNO FARMACEUTICI, grants from ELI LILLY, grants, consultancy and honoraria from KYOWA KIRIN, grants from MSD, grants from NPS, grants and consultant from SERVIER, grants and consultancy from SHIRE, outside the submitted work. BC reports grants and sponsorship from MSD, consultancy for Amgen and occasional interventions for Lilly, Roshe, Ferring and Expanscience. JPP reports personal fees from Mylan, grant and personal fees from TRB Chemedica, outside the submitted work. JMP reports grant and personal fees from TRB Chemedica, outside the submitted work. TT reports personal fees from Abbvie, grants and personal fees from Amgen, personal fees from Arrow, personal fees from Biogen, personal fees from BMS, grants and personal fees from Chugai, personal fees from Expanscience, personal fees from Gilead, personal fees from Grunenthal, grants and personal fees from HAC-Pharma, personal fees from LCA, personal fees from Lilly, personal fees from Medac, grants and personal fees from MSD, grants and personal fees from Novartis, grants and personal fees from Pfizer, personal fees from Sanofi, personal fees from Theramex, personal fees from Thuasne, personal fees from TEVA, grants and personal fees from UCB, grants from Bone therapeutics, outside the submitted work. OB reports grants from Biophytis, IBSA, MEDA, Servier, SMB, Theramex, outside the submitted work. JAK reports grants from UCB, grants from Amgen, grants from Radius Health, outside the submitted work. JYR reports grants and personal fees from IBSA-GENEVRIER, grants and personal fees from MYLAN, grants and personal fees from RADIUS HEALTH, personal fees from PIERRE FABRE, grants from CNIEL, personal fees from DAIRY RESEARCH COUNCIL (DRC), outside the submitted work.
Figures
References
-
- Bruyere O, Cooper C, Pelletier JP, et al. An algorithm recommendation for the management of knee osteoarthritis in Europe and internationally: a report from a task force of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) Semin Arthritis Rheum. 2014;44:253–263. doi: 10.1016/j.semarthrit.2014.05.014. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
