

Circulating matrix metalloproteinases and tissue metalloproteinase inhibitors in patients with idiopathic pulmonary fibrosis in the multicenter IPF-PRO Registry cohort
- PMID: 32171287
- PMCID: PMC7071646
- DOI: 10.1186/s12890-020-1103-4
Circulating matrix metalloproteinases and tissue metalloproteinase inhibitors in patients with idiopathic pulmonary fibrosis in the multicenter IPF-PRO Registry cohort
Abstract
Background: Matrix metalloproteinases (MMPs) and tissue inhibitors of MMPs (TIMPs) play important roles in the turnover of extracellular matrix and in the pathogenesis of idiopathic pulmonary fibrosis (IPF). This study aimed to determine the utility of circulating MMPs and TIMPs in distinguishing patients with IPF from controls and to explore associations between MMPs/TIMPs and measures of disease severity in patients with IPF.
Methods: The IPF cohort (n = 300) came from the IPF-PRO Registry, an observational multicenter registry of patients with IPF that was diagnosed or confirmed at the enrolling center in the past 6 months. Controls (n = 100) without known lung disease came from a population-based registry. Generalized linear models were used to compare circulating concentrations of MMPs 1, 2, 3, 7, 8, 9, 12, and 13 and TIMPs 1, 2, and 4 between patients with IPF and controls, and to investigate associations between circulating levels of these proteins and measures of IPF severity. Multivariable models were fit to identify the MMP/TIMPs that best distinguished patients with IPF from controls.
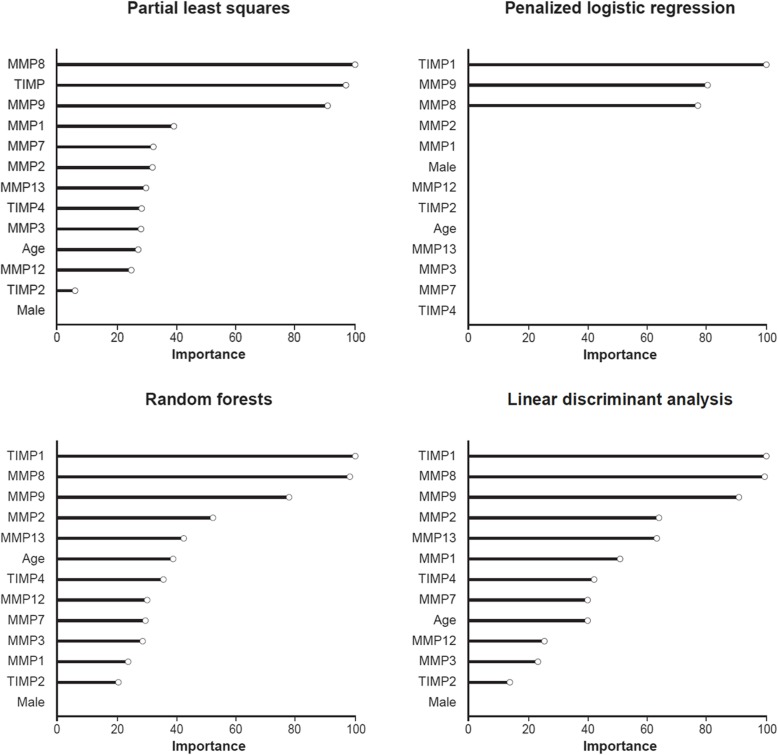
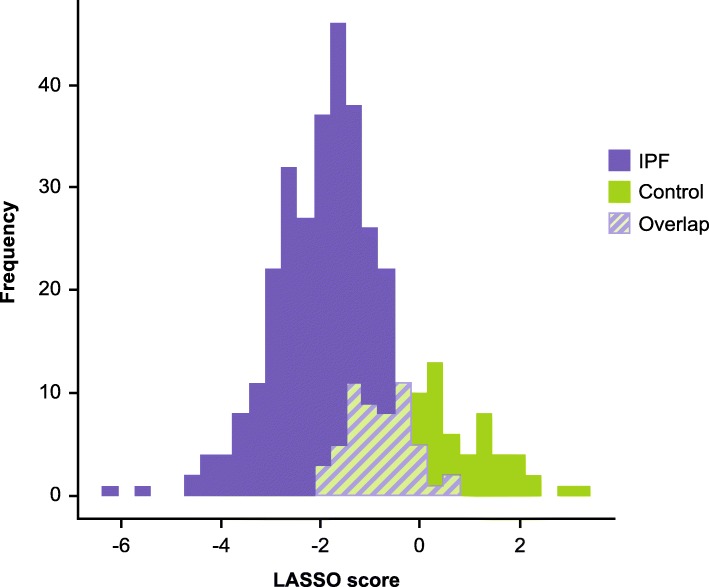
Results: All the MMP/TIMPs analyzed were present at significantly higher levels in patients with IPF compared with controls except for TIMP2. Multivariable analyses selected MMP8, MMP9 and TIMP1 as top candidates for distinguishing patients with IPF from controls. Higher concentrations of MMP7, MMP12, MMP13 and TIMP4 were significantly associated with lower diffusion capacity of the lung for carbon monoxide (DLCO) % predicted and higher composite physiologic index (worse disease). MMP9 was associated with the composite physiologic index. No MMP/TIMPs were associated with forced vital capacity % predicted.
Conclusions: Circulating MMPs and TIMPs were broadly elevated among patients with IPF. Select MMP/TIMPs strongly associated with measures of disease severity. Our results identify potential MMP/TIMP targets for further development as disease-related biomarkers.
Keywords: Biomarkers; Extracellular matrix; Fibrosis; Interstitial lung diseases; Observational study.
Conflict of interest statement
JLT, MLN, RO, LKN and SMP are employees of the Duke Clinical Research Institute, which receives funding support from Boehringer Ingelheim Pharmaceuticals, Inc. to coordinate the IPF-PRO Registry. KRF reports grants and personal fees from Boehringer Ingelheim and Roche/Genentech and personal fees from FibroGen, Sanofi Genzyme, and Veracyte. IN reports personal fees from Boehringer Ingelheim, Genentech and ImmuneWorks. JAL reports personal fees from Boehringer Ingelheim, Roche/Genentech, Galecto, Biogen and Veracyte. MAO reports research grant and grant review fees from Boehringer Ingelheim. RV, KD, YL, CH and TBL are employees of Boehringer Ingelheim. JAB has no competing interests.
Figures



References
-
- Raghu G, Remy-Jardin M, Myers JL, Richeldi L, Ryerson CJ, Lederer DJ, et al. Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2018;198(5):e44–e68. - PubMed
-
- King TE, Jr, Bradford WZ, Castro-Bernardini S, Fagan EA, Glaspole I, Glassberg MK, et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N Engl J Med. 2014;370(22):2083–2092. - PubMed
-
- Richeldi L, du Bois RM, Raghu G, Azuma A, Brown KK, Costabel U, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med. 2014;370(22):2071–2082. - PubMed
-
- Selman M, King TE, Pardo A. Idiopathic pulmonary fibrosis: prevailing and evolving hypotheses about its pathogenesis and implications for therapy. Ann Intern Med. 2001;134:136–151. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
